

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine sarcoma is an uncommon and heterogeneous group of soft tissue sarcoma (STS) with aggressive clinical behavior and poor prognosis [1]. Leiomyosarcoma (LMS) is the most common histological subtype (60%), followed by endometrial stromal sarcoma (ESS), undifferentiated sarcoma, and others. When localized, complete surgical resection of tumors is the treatment of choice whatever the histologic subtype. However, since some patients present with primary metastatic disease and more than half of patients have recurrent metastatic disease after surgery [2], the prognosis of uterine sarcoma remains poor. In metastatic setting, similar to other STS subtypes [3], conventional cytotoxic chemotherapy has shown modest activity against uterine sarcoma.
Pazopanib is an orally-administered, multi-targered tyrosine kinase inhibitor (TKI) with a high affinity for vascular endothelial growth factor receptors (VEGFRs). Based on the results from a pivotal phase III trial [4], pazopanib is currently considered a standard treatment for patients with metastatic, non-adipocytic STS after failure of standard chemotherapy. The anti-tumor activity of pazopanib monotherapy was also evident in Korean STS patients in a retrospective study [5]. Because of oral administration and more favorable toxicity profiles, pazopanib is one of the most widely administered therapy in STS salvage setting. However, when it comes to metastatic uterine sarcoma, an aggressive disease that often shows rapid progression and clinical decline, the clinical trial population might not be indicative of all patients seen in daily oncology practice. When choosing a salvage treatment regimen for an individual patient, factors to be considered include the experiences of the treating oncologists, potential toxicity, especially for those with symptoms or with decreased performance status, as well as the activity of chemotherapeutic agents. Based on these considerations, we designed this single-center, retrospective study to evaluate the efficacy and safety of pazopanib monotherapy in heavily-pretreated, Korean patients with metastatic uterine sarcoma.
MATERIALS AND METHODS
We retrospectively collected and reviewed medical records of 35 adult patients with uterine STS who were consecutively treated with pazopanib (Votrient; GlaxoSmithKline, Research Triangle Park, NC, USA) as salvage therapy in between September 2013 and December 2015. Patients enrolled in clinical trials were excluded to ensure the study population reflected our daily clinical practice, and the choice of pazopanib was solely at the discretion of the treating oncologists. Other exclusion criteria for case inclusion were as follows: 1) absence of measurable metastatic disease, 2) histologic diagnosis of osteosarcoma, chondrosarcoma, liposarcoma, Ewing's sarcoma, primitive neuroectodermal tumor, or other excluded subtypes in the pazopanib phase III trial [4], 3) another malignancy within 5 years, and patients with inappropriate laboratory findings or severe comorbid illness for standard 800 mg per day dose of pazopanib. Institutional Review Boards approval was obtained from Samsung Medical Center (SMC; Seoul, Korea). Written informed consent was given by all patients prior to starting pazopanib, according to institutional standards.
In all patients, pazopanib at a starting dose of 800 mg per day was administered orally without interruption. Supportive care including the administration of blood products, and the use of analgesics was given if judged appropriately by the treating physicians. Before initiating the first dose of pazopanib, patients had a complete history taken, complete blood counts and serum chemistries, chest X-rays, and computed tomography scans of all involved sites. Patients were seen every 4 weeks as pazopanib therapy was repeated every 4 weeks. Therapy was continued until objective disease progression per Response Criteria in Solid Tumours (RECIST) [6], unacceptable toxicity or deterioration of hepatic function, or patient refusal. Dose adjustments at the start of a new cycle were based on the worst toxicity observed during the previous cycle. Baseline characteristics and outcome data were collected using a uniform case report form. Clinical and laboratory parameters collected at the time of starting pazopanib included age, Eastern Cooperative Oncology Group (ECOG) performance status, histological grade according to Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC), site(s) of metastases, previous surgery and/or radiotherapy, and previous chemotherapeutic regimens. Responses were evaluated every 8 weeks by chest and abdominopelvic computed tomography or by the same tests that were used to stage initial tumors. Adverse events were collected and graded according to the National Cancer Institute criteria (Common Terminology Criteria for Adverse Events [CTCAE] v4). To determine the causes of death, as well as therapy discontinuation, a structured medical record review was performed.
The primary end point was the response rate (RR). Secondary end points included progression-free survival (PFS), overall survival (OS), and a toxicity profile. Time from the first day of pazopanib administration to death, whatever the cause, was used to calculate OS. PFS and OS were calculated using the Kaplan-Meier method. To examine the impact of baseline parameters collected on PFS and OS, Cox proportional hazard model was used. Laboratory parameters and age were initially recorded as continuous variables, and evaluated as both continuous and categorical variables. The potential presence of interaction effects between baseline parameters was tested by defining product terms for the respective factors in a regression model. All p-values were 2-sided, with p<0.05 indicating statistical significance. All analyses were performed using the R for Windows v2.11.1 software (R Core Team, Vienna, Austria; http://www.Rproject.org).
RESULTS
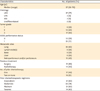
The SMC cancer chemotherapy registry identified 35 eligible patients who were treated with salvage pazopanib for metastatic STS of uterine origin. Patient characteristics are given in Table 1. As shown, their median age was 57 years (range, 36–70). Approximately 77% of patients had a histologic diagnosis of LMS, followed by undifferentiated pleomorphic sarcoma (UPS), ESS, and undifferentiated sarcoma. Patients with ESS (n=3) had a high-grade (FNCLCC grade 3/3) tumor. All patients were heavily pretreated, as half of them had received 2 or more chemotherapy regimens. Because of the lack of a standard therapy for STS, prior chemotherapy regimens included etoposide/ifosfamide/cisplatin (n=15), docetaxel/gemcitabine (n=14), doxorubicin monotherapy (n=9), doxorubicin/cisplatin (n=7), ifosfamide monotherapy (n=6), and doxorubicin/ifosfamide (n=4). Most commonly involved site of metastases was lung, retroperitoneum, and/or peritoneum. At the time of data collection, with a median follow-up duration of 34 months, 29 patients developed disease progression and 22 had died.
Table 1
Baseline characteristics of all 35 patients
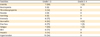
A total of 229 4-week pazopanib cycles were administered (median 4, range 1–24). The most common reason for therapy discontinuation was disease progression (80%). Overall, oral pazopanib was generally well tolerated, with hypertension, stomatitis, fatigue and grade 1 or 2 anemia being the most commonly observed toxicities (Table 2). Transient and reversible liver function test elevation was observed in 5 patients. No treatment-related deaths were identified.
Table 2
Maximum grade toxicity recorded per patient (n=35)
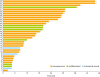
Of a total of 35 patients, one patient could not be evaluated for clinical responses because of early discontinuation of therapy. Objective responses to pazopanib were noted in 10 patients (RR=29%; 95% confidence interval [CI]=14%–44%), including one complete response. Stable disease was observed in 11 patients (31%), leading to a 60% disease control rate (Fig. 1). Patients who had a LMS histology were, although statistically insignificant (p=0.80), more likely to respond to pazopanib (9/27, 33%) compared to those with UPS (1/3, 33%) or ESS (0%). In addition, to explore predictive factors for clinical response to pazopanib, we performed a logistic regression analysis with known baseline parameters. As a result, RR was not significantly influenced by histologic subtypes (LMS vs. non-LMS; odds ratio [OR]=0.79; 95% CI=0.13–4.79; p=0.79), age (>median vs. ≤median; OR=0.91; 95% CI=0.19–4.48; p=0.91), performance status (0 vs. 1; OR=0.78; 95% CI=0.18–3.42; p=0.74), FNCLCC grade (1 or 2 vs. 3; OR=0.58; 95% CI=0.14–2.50; p=0.46), number and site of metastases, or baseline laboratory parameters. We also tested whether the development of clinical responses was modified by interaction between the effects of parameters; the first-level interaction term between these variables was entered into separate multivariate model but we found no interaction between them.

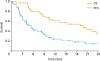
The estimated median PFS and OS were 5.8 months (95% CI=3.6–8.1) and 20.0 months (95% CI=11.6–28.4), respectively (Fig. 2). In contrast to RR, within the limitation of small sample size, the estimated PFS (median 5.8 months, 95% CI=2.5–9.1 vs. 3.0 months, 95% CI=0–7.6; p=0.680) as well as OS (20.0 months vs. not reached; p=0.404) were similar between patients with LMS and ESS or other histologic subtypes, respectively (Fig. 3). In the Cox regression model, the estimated PFS or OS was not significantly influenced by any of the baseline parameters. After pazopanib failure, half (49%) of the patients received further lines of therapy, mostly with taxane-based (n=14) and clinical trials with novel agents (n=10). For exploratory purposes, we then compared OS between patients who received further therapy after pazopanib failure and who did not. Although statistically insignificant, those who received further lines of therapy lived longer (27.4 vs. 8.6 months, p=0.156).
DISCUSSION
This retrospective study on a limited number of patients showed that the salvage therapy with pazopanib in Korean patients with uterine STS can be both well tolerated and active, regardless of their performance status or the number of metastases. The estimated median PFS and OS were 5.8 months (95% CI=3.6–8.1) and 20.0 months (95% CI=11.6–28.4), respectively. Most cases of adverse events were transient and self-limited. In addition, there were few severe non-hematologic toxicities, with grade 3 or 4 stomatitis or diarrhea in only 3%–6% of patients. The results compared favorably with outcomes obtained in prospective clinical trials [24], as well as a Korean retrospective study [5]. However, the clinical benefit with pazopanib was limited to patients with LMS. In those with uterine LMS, pazopanib achieved objective response in 33% of patients, whereas 13% in other histologic subtypes. Although this study is retrospective in nature and has a limited number of patients, our results seem to suggest that patients with uterine STS other than LMS may not derive clinically relevant benefit from treatment with pazopanib.
Uterine STS is an uncommon but aggressive mesenchymal tumor. Because of the relative rarity of uterine STS, clinical decision making depends on data available for STS arising from other primary sites [7]. In metastatic setting, active agents against STS include doxorubicin, ifosfamide, taxanes, gemcitabine, and trabectedin. Pazopanib, an orally-administered VEGFR TKI, has been the mainstay of therapy in the treatment of non-adipocytic STS patients failing prior chemotherapy, on the basis of the prospective phase II and III trials [24]. These 2 clinical trials included a total of 44 patients with uterine STS, and the results of a subgroup analyses was recently published [8]. Although the authors concluded that the clinical efficacy of pazopanib in patients with uterine STS was comparable to those with non-uterine STS, a majority (89%) of patients had LMS histology. In the present study, we observed that other subtypes of uterine STS than LMS, ESS or undifferentiated sarcoma in particular, did not respond to pazopanib. These histologic subtypes probably differ both clinically and biologically, but it remains unknown if there are any clinical or biologic characteristics that would result in pazopanib unresponsiveness.
The best choice of treatment regimen for patients with metastatic STS is still a matter of controversy and requires careful considerations of individual patient's disease status, symptoms, general condition, and histologic subtype. In first-line setting, the decision to use chemotherapeutic agents, alone or in combination should be determined by their relative merits on a case-by-case basis [39]. More recently, more than a few targeted agents have shown promising results in patients with metastatic STS. In addition to pazopanib, a novel monoclonal antibody olaratumab that blocks platelet-derived growth factor receptor (PDGFR) showed improved survival when combined with doxorubicin [10]. Although we do not know how many patients with uterine STS were included in the olaratumab trial, the subsequent phase III trial (ANNOUNCE; ClinicalTrials.gov, NCT02451943) is under way so that the final results are awaited.
The strength of this study includes its single-center nature with patients who were treated with pazopanib as a routine clinical practice to avoid selection bias. It should be noted that the patients included in this study are consecutive series of patients taken from an academic, tertiary cancer center to reflect the real-world experience of salvage pazopanib. This indeed may differ from clinical trial patients, which is more relevant to the clinician's daily practice. That is, the study reflects real-world outcomes that may not necessarily be seen in randomized controlled trials with selected patients. On the other hand, limitations of this study include its retrospective nature, which may predispose the study to selection bias and issues with missing data. Selection bias can be minimized by obtaining consecutive series of patients as seen in the current results. The lack of central radiology review, variable modalities of imaging, and intervals between scans were potential weaknesses; however, we believe it better reflects the real-world experience of oncologists treating patients with uterine STS.
In conclusion, results obtained in the present study suggest that pazopanib is an active and safe regimen for the salvage therapy of Korean patients with uterine STS. Although it is encouraging that OS and PFS for Korean patients with uterine STS were similar to those reported in the phase III trial, the clinical benefit was limited to those with LMS. With better patient selection, clinical outcomes of patients with pretreated, metastatic, uterine STS can be improved.
 XML Download
XML Download