

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lynch syndrome is a cancer predisposition syndrome caused by germline mutation of DNA mismatch repair (MMR) genes MLH1, MSH2, MSH6 and PMS2 [1]. It is an autosomal dominant syndrome with an elevated risk of colorectal, endometrial, ovarian and other cancers. Lynch syndrome accounts for 2%–6% of endometrial cancer and the cumulative lifetime risk of endometrial cancer in female carriers of Lynch syndrome is about 28%–60%, depending on which gene is mutated [23]. However, Lynch syndrome is thought to be less common in ovarian cancer and accounts for 0.4%–1% of cases of ovarian cancer [456]. The cumulative lifetime risk of ovarian cancer for women with Lynch syndrome is 6%–14% [78], while the risk of ovarian cancer in the general population is about 1.6%. These associations between ovarian cancer and Lynch syndrome are unclear in the Asian population.
Traditional screening for Lynch syndrome uses a two-step approach using clinical criteria based on a patient's clinical and family history of cancer and molecular tests for microsatellite instability (MSI) or immunohistochemistry (IHC). The Amsterdam II criteria and revised Bethesda guidelines are well-known clinical criteria. The Amsterdam II criteria are particularly stringent: half of families who meet these criteria have a MMR gene mutation, but the criteria may miss 68% of patients with Lynch syndrome [9]. In contrast, the revised Bethesda guidelines have better sensitivity, with 72%–88% of Lynch syndrome patients meeting the guidelines, but still fail to detect many patients with Lynch syndrome [10]. These problems with clinically based criteria led to development of an alternative strategy of universal screening, in which all patients with newly diagnosed colorectal cancer undergo a MSI test or IHC. This approach has high sensitivity and is cost-effective in patients with colorectal cancer. Universal screening for patients with endometrial cancer is also becoming a standard practice [1112].
The screening strategy for Lynch syndrome patients with ovarian cancer is controversial. Universal screening may provide high sensitivity, but may not be cost-efficient unless performed in cases at high risk for Lynch syndrome because of the low incidence of Lynch syndrome in ovarian cancer. The Amsterdam II criteria do not include ovarian cancer as a Lynch-associated cancer and the revised Bethesda guidelines are mainly focused on colorectal cancer; therefore, these criteria are not useful for selection of patients with ovarian cancer who are at high risk for Lynch syndrome. In this study, we examined an alternative screening strategy for Lynch syndrome using risk assessment criteria based on the clinical and family history of patients with ovarian cancer.
MATERIALS AND METHODS
1. Subjects
The subjects were 129 patients with epithelial ovarian cancer who were treated as outpatients or inpatients at our hospital from April 2015 to August 2016. Outpatients were previously diagnosed and treated for ovarian cancer and followed at our clinic. Inpatients were hospitalized for surgery for ovarian cancer. The eligibility criteria were female gender, diagnosis of ovarian cancer, and age ≥20 years old. All patients gave written informed consent and the study was approved by the Institutional Review Board (approval number: 2007-0081). Clinical and family cancer history were collected from patients using a self-administered questionnaire. This self-administered questionnaire can collect family history for 3-degree relatives and we previously reported about this questionnaire [13]. Information from these questionnaires was collected in our biobank database, together with clinical and pathological data from medical records. The genetic risk for Lynch syndrome was assessed using the questionnaire data based on SGO criteria (SGO statement on risk assessment 2007; 5%–10% chance for having Lynch syndrome [14]) (Table 1). Use of the SGO criteria based on clinical and family history allowed identification of patients with a genetically high risk for Lynch syndrome. Patients who met at least one criterion were classified as high risk (SGO-positive), and then underwent a MSI test, IHC for MMR proteins (MLH1, MSH2, MSH6, and PMS2), and evaluation of methylation of promoter regions of MMR genes (MLH1, MSH2, and MSH6) by methylation-specific polymerase chain reaction (MSP). Samples from cancer and non-cancer regions of the ovary used in these analyses were obtained from paraformaldehyde-fixed, paraffin-embedded surgical samples. Genetic counseling and testing were recommended for patients who were positive for MSI or IHC and were suspected to have Lynch syndrome.
Table 1
SGO criteria (SGO statement on risk assessment 2007; 5%–10% chance for having Lynch syndrome)

HNPCC, hereditary nonpolyposis colorectal cancer; SGO, Society of Gynecologic Oncology.
*Lynch/HNPCC-related tumors include colorectal, endometrial, stomach, ovarian, pancreas, ureter and renal pelvis, biliary tract, and brain (usually glioblastoma as seen in Turcot syndrome) tumors, sebaceous gland adenomas and keratoacanthomas in Muir-Torre syndrome, and carcinoma of the small bowel; †First and second degree relatives are parents, siblings, aunts, uncles, nieces, nephews, grandparents and grandchildren.
![]()
The risk for Lynch syndrome was also examined using PREMM5 (PREdiction Model for gene Mutations) [15], which estimates the cumulative probability of having an MLH1, MSH2, MSH6, PMS2, and EPCAM mutation based on personal and family history. PREMM5 sets the cut-off as ≥2.5% and recommends for further tumor tests. We used this prediction model as a comparison with SGO criteria in this research.
2. Microsatellite instability analysis
To detect loss of function in MMR, MSI was evaluated by FALCO Biosystems for 5 satellite markers: NR21, NR24, BAT25, BAT26, and MONO27 (Promega, Madison, WI, USA). Tumors showing an allelic shift of two or more markers were defined as high MSI (MSI-H), those with an allelic shift of one marker as low MSI (MSI-L), and those with no allelic shift at any marker as microsatellite stable (MSS).
3. Immunohistochemistry
Immunohistochemical analysis was performed as previously described [16]. Tissue was fixed overnight with 4% paraformaldehyde, embedded in paraffin, and prepared as sections of 4 μm. Sections depleted of paraffin were immunostained with primary antibodies against MLH1 (M3640), MSH2 (M3639), MSH6 (M3646), and PMS2 (M3647) followed by peroxidase-conjugated secondary antibodies (ENVISION+; all Dako, Santa Clara, CA, USA). Sections were counterstained with hematoxylin to visualize cell nuclei. The staining results were independently evaluated by 2 trained investigators.
4. Methylation analysis
The methylation status of CpG islands in the MLH1, MSH2 and MSH6 promoters was analyzed by MSP. This method detects methylation of bases by a bisulfite reaction and subsequent detection by polymerase chain reaction (PCR) with primers specific to bisulfite-converted methylated and unmethylated sequences [1617]. MSP primer sets for MLH1, MSH2, and MSH6 are summarized in Supplementary Table 1. CpGenome Universal Methylated DNA and Unmethylated DNA (Millipore, Temecula, CA, USA) were used as the respective positive controls for methylated and unmethylated PCR.
5. Germline mutation analysis
Mutation screening of MMR genes was performed by direct sequencing [18]. Genetic test was performed for MLH1/MSH2/MSH6, and PMS2. RT-PCR/direct sequencing was performed, and we confirmed the mutation by direct sequencing using genome DNA in MLH1 and MSH2. Also, we checked large rearrangement by multiplex ligation-dependent probe amplification (MLPA) for MLH1/MSH2MSH6 and PMS2.
RESULTS
Of the 129 cases of ovarian cancer, 25 (19.4%) met the SGO criteria 2007, and thus had a 5%–10% risk for having Lynch syndrome. One case met the revised Bethesda guidelines and there were no case who met Amsterdam II criteria. However, there was a patient whose family member met Amsterdam II criteria. Among the 25 genetically high-risk cases, 15 were identified only from a criterion of a first- or second-degree relative meeting the above criteria (Table 1) in the family history of cancer. There was no significant difference in age, body mass index (BMI), histological type of cancer, and stage of diagnosis between the groups with genetically high and low risks for Lynch syndrome (Table 2). The 25 SGO-positive cases included 13 with ovarian cancer only, 9 with synchronous ovarian and endometrial cancer, and 3 with ovarian cancer accompanied by breast cancer, colorectal cancer, and atypical endometrial hyperplasia in one case each. These pathological results were diagnosed and reviewed by more than 2 well-trained pathologists. Also, these diagnosis and pathological reports were double checked by gynecologic doctor for confirmation. The diagnosis of synchronous ovarian and endometrial cancer and distinguish of metastasis was based on Ulbright and Roth criteria and Scully's definition [1920]. Detail of these 25 cases who met SGO criteria were shown in Table 3 (family history is shown in Supplementary Table 2).
Table 2
Characteristics of patients at genetically high risk (meeting SGO criteria) and low risk (not meeting SGO criteria) for Lynch syndrome
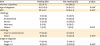
Values are presented as number of patients (%) or mean±standard deviation.
BMI, body mass index; SGO, Society of Gynecologic Oncology.
*t-test, †Pearson χ2 test.
![]()
Table 3
Details of 25 cases that met SGO criteria

Colored column showed the cases who are suspected Lynch syndrome.
AC, Amsterdam II criteria; AEH, atypical endometrial hyperplasia; BC, breast cancer; CC, colorectal cancer; EC, endometrial cancer; IHC, immunohistochemistry; M, methylated; MSI, microsatellite instability; MSI-H, high MSI; MSP, methylation-specific polymerase chain reaction; MSS, microsatellite stable; OC, ovarian cancer; rBG, revised Bethesda guidelines; SGO, Society of Gynecologic Oncology; U, unmethylated.
![]()
Four of the 25 SGO-positive cases were MSI-high, and these 4 cases also had loss of expression of MMR protein: 2 with loss of MSH2 and MSH6 (cases 11 and 24), and 2 with loss of MLH1 and PMS2 (cases 17 and 23). Both cases with loss of MSH2 and MSH6 were suspected to be Lynch syndrome with MSH2 mutation. In the 2 cases with loss of MLH1 and PMS2, one (case 17) had promoter methylation in MLH1, indicating sporadic ovarian cancer, and another (case 23) had no methylation, indicating MLH1 mutation. Therefore, cases 11, 23, and 24 had suspected Lynch syndrome (3/25, 12.0%) and genetic counseling and genetic testing were recommended for these patients. These 3 cases did not meet the Amsterdam II criteria or revised Bethesda guidelines, but met SGO criteria. Family trees and IHC of these cases are shown in Fig. 1. After sufficient genetic counseling, the patient in case 24 (synchronous ovarian and endometrial cancer with loss of MSH2 and MSH6) decided to undergo genetic testing. Germline genetic analysis revealed a nonsense mutation in MSH2 and she was diagnosed as Lynch syndrome. The other two patients with suspected Lynch syndrome are currently refusing to undergo genetic counseling.
 | Fig. 1Immunohistochemistry of ovarian cancer tissue and family tree in 3 cases with suspected Lynch syndrome. (A) Case 11: endometrioid carcinoma grade 2 with loss of MSH2 and MSH6. She had young onset of OC, with family cancer history of EC and CC. (B) Case 23: endometrioid carcinoma grade 2 with loss of MLH1 and PMS2. She had synchronous EC and OC, with family cancer history of EC and CC. (C) Case 24: endometrioid carcinoma grade 1 and clear cell carcinoma with loss of MSH2 and MSH6. She had synchronous EC and OC, with family cancer history of CC and GC.
CC, colorectal cancer; EC, endometrial cancer; GC, gastric cancer; OC, ovarian cancer
|
The risk of Lynch syndrome was checked by PREMM5, which calculates this risk based on personal and family history. By PREMM5, 31 patients were positive for high risk, 13 patients were SGO-negative and other 18 patients were SGO-positive. Cases 11, 23, and 24 were positive in PREMM5. However, overall there were some differences between the SGO risk assessment and PREMM5 risk prediction (Table 4): 7 of 25 SGO-positive cases (28.0%) were PREMM5-negative, and 13 of 104 SGO-negative cases (12.5%) were PREMM5-positive. The calculated risk of these 13 patients who were negative for SGO criteria but positive for PREMM5 were all low (2.5%–5.0%).

DISCUSSION
The goal of this study was to investigate a screening strategy to detect Lynch syndrome in patients with ovarian cancer, based on the idea that risk assessment using personal and family history may be cost-effective in these patients due to the low incidence of Lynch syndrome in ovarian cancer. One patient in whom Lynch syndrome was subsequently confirmed and 2 candidate patients were detected in 129 cases (2.3%) of patients with ovarian cancer, and this rate was increased to 12.0% (3/25) by targeting the high-risk group based on SGO criteria. The rate of 12.0% is appropriate because the SGO criteria are designed to select patients who have a greater than 5%–10% risk of having Lynch syndrome.
Targeting high-risk cases, instead of using universal screening, is important in the screening strategy for Lynch syndrome in ovarian cancer. The Amsterdam II criteria do not include ovarian cancer as a Lynch-associated cancer and the revised Bethesda guidelines are focused on colorectal cancer. Therefore, we focused on SGO criteria to investigate the screening strategy. There is a report that using SGO criteria as a clinical screening can detected Lynch syndrome better than Amsterdam II criteria or revised Bethesda guidelines in endometrial cancer patients; SGO 5%–10% risk assessment criteria can select 93% of Lynch-associated endometrial cancer, whereas Amsterdam II criteria and revised Bethesda guideline can select only 36% and 58% [21]. However, the sensitivity and specificity of SGO criteria to identify Lynch syndrome in unselected endometrial cancer cases was reported as 32.6% and 77%, they concluded universal screening is recommended in patient with endometrial cancer [22]. Applying the SGO criteria for ovarian cancer is not well studied. Chui et al. [23] showed that the proportion of the patients who have ovarian cancer with Lynch syndrome and fulfilled clinical criteria based on Amsterdam II criteria, revised Bethesda guidelines and SGO 5%–10% risk assessment was 45%, 50%, and 80% respectively, indicating the efficacy of SGO criteria for screening of Lynch syndrome in ovarian cancer patients. However, the original SGO criteria were updated in 2015 [24]; these updated criteria are based on universal screening (Supplementary Table 3). Furthermore, these updated criteria do not include ovarian cancer. That why we did not focus on SGO criteria 2015. The 2007 SGO criteria are not so restricted and include ovarian cancer as a Lynch-associated cancer in personal and family history. Therefore, these criteria seem to be most appropriate for screening for Lynch syndrome in ovarian cancer patients.
There were some differences in results based on SGO criteria and those for the risk of Lynch syndrome estimated by PREMM5, which calculates the risk as a percentage. PREMM5 is mainly focused on colorectal cancer and endometrial cancer, and this may explain why some SGO-positive cases were negative in PREMM5. Also, PREMM5 uses a cut-off of >2.5% for recommendation of a further test for Lynch syndrome, whereas the SGO criteria assess the 5%–10% risk of Lynch syndrome, and this may cause some SGO-negative cases to be PREMM5-positive. As shown in results, these SGO-negative but PREMM5-positive cases were thought to have lower risk because calculated risk were all low (2.5%–5.0% risk). However, PREMM5 is a good model for percentage risk assessment and the three cases of suspected Lynch syndrome in our study were all PREMM5-positive. It is difficult to conclude which risk assessment is better; however, the SGO criteria seem to be sensitive for detection of Lynch syndrome in ovarian cancer because SGO criterion (e) can pick up the patients who have high risk family member. One limitation of this study is that we could not perform MSI testing and IHC in SGO-negative cases, and thus we do not know if there were false-negative cases in our findings. However, based on the rate of 0.4% for Lynch syndrome in all ovarian cancer cases, and considering that 3 of 129 cases (2.3%) in our study were suspected to have Lynch syndrome and one case (0.78%) was diagnosed as Lynch syndrome, it is unlikely that any patients with Lynch syndrome were included in the SGO-negative cases. Another limitation is that we cannot performed genetic test to other two cases of MSI-H and loss of expression of MMR protein and other cases who met SGO criteria, especially who met revised Bethesda guidelines. We cannot declare whether other two cases of abnormal tumor test have germline mutation, however it is important that MSI-H and loss of MMR expression cases were effectively extracted, and this screening procedure might help for further researches including target therapy of anti-programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PDL-1) for MSI-H tumors.
The three cases of suspected Lynch syndrome all had a histopathological type of endometrioid carcinoma and it is consistent to previous reports that Lynch-associated ovarian cancer tends to be non-serous carcinoma [52526]. The frequency of loss of MMR (3.1%; 4/129) is also similar to that in a study of MMR deficiency in cases of unselected ovarian cancer [26]. Focusing on cases of endometrioid and clear cell ovarian carcinoma or young onset (<50 years old) seems to be effective for detecting loss of MMR and Lynch syndrome [2728], while our results indicate that screening using clinical and family history is also effective.
The frequency of MSI was 3.1% (4/129) in this study, which is lower than previous reports [29]. It is unclear whether MSI is a reliable proxy for loss of MMR in ovarian cancer. Some studies have identified MSI-H in more than 60% of ovarian epithelial tumors, while MMR protein expression was intact in a subset of these cases [30], and MSI is also found in more than 50% of normal ovarian tissues [3031]. Other studies have found a lower MSI-H frequency of 10%–20% [2732]. These differences may depend on the patient population and evaluation method. In fact, we used different MSI markers to those recommended by the National Cancer Institute and this may have caused a discrepancy in MSI status in this study.
It is well-known that serous ovarian cancer is the most common histological type in western country and endometrioid and clear cell carcinoma is more common in Asia, especially in Japan. Recent reports showed that 42.3% of ovarian cancer was endometrioid or clear cell carcinoma and it was increasing in this decade in Japan [33]. The frequency of endometrioid or clear cell carcinoma was relatively high (58.9%; 75/129) in this research. It may be due to small sample size and high frequency of endometrioid endometrial and ovarian double primary cancer. This synchronous or metachronous endometrial and ovarian cancer is known to show endometrioid histological type in more than 50%–80% cases [343536]. We had 7.0% (9/129 cases) of synchronous or metachronous endometrial and ovarian cancer in this research and it is similar to previous report that synchronous endometrial and ovarian cancer is account for 10% of all ovarian cancer patients [37]. Also, previous reports showed that Lynch syndrome is included in about 10% of synchronous endometrial and ovarian cancer [343839]. There is no contradiction that 2 of 9 synchronous and metachronous endometrial and ovarian cancer patients showed abnormal MSI and IHC test and one case showed MSH2 germline mutation. This synchronous or metachronous endometrial and ovarian cancer is difficult to diagnose even it is based on Ulbright and Roth criteria and Scully's definition. Recent investigation showed the genetical clonality of clinically diagnosed synchronous endometrial and ovarian cancer, indicating single primary tumor with metastasis [40]. Considering a relative high frequency of synchronous endometrial and ovarian cancer in patients with genetically high risk of Lynch syndrome, we must carefully diagnose ovarian cancer whether it is primary or metastatic to assess the risk of Lynch syndrome correctly.
In conclusion, this is the first investigation of screening for Lynch syndrome in ovarian cancer using clinical and family history in an Asian population. Diagnosis using this method may be effective for detecting Lynch syndrome in patients with ovarian cancer.
 XML Download
XML Download