

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The population of single women has steadily increased over the past 4 decades in the United States. In 2016, more than half of women over the age of 25 had never been married [1]. In addition, single marital status has been associated with an increased risk of mortality for various types of malignancies [2345]. However, population-based trends of marital status among women with malignancy of the uterine cervix have not been well examined.
Cervical malignancy is ranked as the fourteenth most common malignancy in women in the United States, with an estimated 12,820 new cases and 4,210 deaths in 2017 [6]. There has been a 57% decrease in the age-adjusted incidence between 1975 and 2013 [7]. This drastic decrease in incidence is due to both advances in cervical cancer screening and development of human papillomavirus (HPV) vaccines [89]. Cervical cancer screening provides an opportunity for early detection of malignancy, as well as for treatment of cervical dysplasia before cancer develops. Patient compliance with cervical cancer screening recommendations is tantamount in order for prevention via screening to be effective.
A previous study demonstrated that one of the factors influencing the utilization of cervical cancer screening in the United States is marital status [10], and women with single marital status are less likely to utilize cervical cancer screening and are more likely to have greater risk for HPV infections, as indicated by a higher prevalence in this population [11]. In this study, we aimed to examine trends, characteristics, and outcomes of single women with cervical malignancy.
MATERIALS AND METHODS
1. Study design and eligibility
A retrospective observational study was conducted to examine the Surveillance, Epidemiology, and End Results (SEER) program, a population-based tumor registry launched in 1973 in the United States. This database was initiated in 5 States and 2 areas and now covers approximately 27.8% of the US population from 11 states and 7 areas [12]. The Institutional Review Board in our institution exempted this study due to use of publicly available de-identified data. SEER*Stat 8.3.2 was used to sort the dataset. A total of 12 female malignancies including the 10 most common malignancies as well as the 2 most common gynecologic malignancies were searched between 1973 and 2013. These malignancy types included breast, lung/bronchus, colon, uterine corpus, thyroid, non-Hodgkin lymphoma, melanoma, kidney, pancreas, leukemia, ovary, and uterine cervix. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were utilized for this study [13].
2. Clinical information
Patient demographics abstracted included the age at diagnosis (<40 vs. ≥40 years), year of diagnosis (1973–1979, 1980–1989, 1990–1999, 2000–2009, and 2010–2013), race/ethnicity (White, Black, Hispanic, Asian, and others), registration area (west, central, and east), and insurance status (yes, no, or unknown). In the SEER database, marital status at the time of malignancy diagnosis was defined as follows; single, never married; married, including common law; separated; divorced; widowed; unmarried or domestic partner, same sex or opposite sex, registered or unregistered; and unknown. The SEER tumor registry defined marital status at disease diagnosis, and coding for single marital status in this database indicates no previous marriage prior to the diagnosis of malignancy.
Tumor characteristics included histologic subtype (squamous, adenocarcinoma, adenosquamous, or others), stage (I, II, III, or IV), grade (1, 2, or 3), and tumor size (≤2.0, 2.1–4.0, or >4.0 cm). In this study, the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) SEER Site/Histology Validation List and the World Health Organization histological classifications were used for grouping histologic subtypes [14]. Per the SEER data coding system, stage was reclassified according to the American Joint Committee on Cancer 7th Edition staging criteria [15]. Treatment patterns included use of hysterectomy, regional lymph node removal, and postoperative radiotherapy.
3. Statistical analysis
The primary objective was to examine time-trends surrounding the proportion of women with single marital status across the 12 malignancy types. The secondary objective was to investigate characteristics of single marital status women with malignancy of the uterine cervix. In addition, the associations of age and single marital status were examined.
Continuous variables were assessed by Student's t-test or Mann-Whitney U test, expressed as a mean (±standard deviation) or median (range) as appropriate. Ordinal and categorical variables were analyzed using the χ2 test. A binary logistic regression model was used to identify independent contributing factors for single marital status. Patient demographics, tumor characteristics, and treatment approaches were entered in the final model. Magnitudes of statistical significance were expressed with adjusted odds ratio (OR) and 95% confidence interval (CI).
The Joinpoint Regression Program (version 4.3.1.0) provided by the National Cancer Institute was utilized for evaluating temporal trends of the proportion of women with single marital status and the proportion of women aged <40 years at diagnosis of malignancy [16]. Time point data were examined every calendar year to identify temporal changes. The presence of an annual trend was examined with a linear segmented regression test, and log-transformation was performed to determine the annual percentage rate change (APC) and 95% CI. All statistical tests were 2-tailed, and a p-value of less than 0.05 was considered to be statistically significant. Statistical Package for the Social Sciences (version 24.0; IBM SPSS, Armonk, NY, USA) was used for all the analyses.
RESULTS
1. Patient demographics
There were 3,294,208 cases of the 12 target malignancies during the study period (Table 1). Breast (n=1,210,332) was the most common site of the malignancy followed by lung (n=475,961), colon (n=439,782), and uterine corpus (n=235,849). The uterine cervix was the eleventh most prevalent site of malignancy (n=87,151). There were 415,715 single marital status women with malignancy diagnoses within the 12 examined (12.6%), and the proportion of the single women was different among the 12 malignancies. Malignancy of the uterine cervix included the highest proportion of single marital status women among the examined malignancy sites (21.2%). The mean age of women with the 12 malignancies was 61.9 years. Women with thyroid malignancy had the youngest mean age (48.1 years), followed by malignancy of the uterine cervix (50.9 years).
Table 1
Patient demographics of 12 female malignancies (n=3,294,208)

2. Factors associated with single women in malignancy of the uterine cervix
Patient demographics and contributing factors for single marital status in malignancy of the uterine cervix are shown in Table 2. The majority of these cases were under 40 years, of Caucasian ethnicity, western regional residency, and diagnosed after 2000. The majority of these tumors were squamous cell carcinoma histological subtype, high-grade, and were of a larger tumor size (>4 cm). On multivariable analysis, single marital status was independently associated with younger age, Black/Hispanic ethnicity, western registry residency, uninsured status, more recent diagnosis, advanced-stage disease, non-adenocarcinoma histology, higher tumor grade, and large tumor size. Treatment for single women was less likely to include hysterectomy compared to other counterparts (all, adjusted p<0.05). In an attempt to examine the association of marital status and tumor characteristics, sensitivity analysis was performed with known information on tumor histology, grade, size, and stage (Supplementary Table 1). This analysis essentially re-demonstrated the aforementioned association indicating that single marital status was independently associated with non-adenocarcinoma histology and large tumor size (all, adjusted p<0.05).
Table 2
Patients demographics and contributing factors for single marital status with cervical malignancy (n=87,151)

Number (%) or mean±standard deviation is shown. A binary logistic regression model for multivariable analysis (ORs for single marital status). All patient factors and tumor characteristics, and treatment patterns were entered in the final model. Others including married, separated, divorced, widowed, unmarried or domestic partner, and unknown.
CI, confidence interval; OR, odds ratio.
*Undifferentiated grade.
3. Trends of single women with malignancy of the uterine cervix
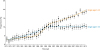
The proportion of single women among those with malignancy of the uterine cervix was 6.3% in 1973 which was the third lowest among the 12 malignancies. In the next 40 years, the proportion of single women significantly increased in all the examined malignancies (Fig. 1A). Notably, this interval increase in the proportion of single women was particularly prominent in cervical malignancy, and there was a significant surge in the proportion of single women with cervical malignancy starting in the early 1990s, exhibiting the largest APC among all the examined malignancies (1.8%; 95% CI=1.6, 2.0; p<0.001). By 2013 it had reached nearly 30% (29.3%) which was far higher than any other malignancy. Women with thyroid malignancy had the second highest proportion of single marital status (21.1%), followed by leukemia (20.8%), and ovarian malignancy (20.8%) in 2013.
Fig. 1
Time-trends of proportion of single women and young age women in the United States.
Results of piecewise linear regression analyses by Joinpoint Regression Program were shown to display temporal trends of the proportion of women with single marital status (A) and the proportion of women with aged younger than 40 years at the time of diagnosis of malignancy (B) in 12 female malignancies between 1973 and 2013 (dots represent actual observed value, and lines represent regression curves for modeled values).

4. Association of age and single women in malignancy of the uterine cervix
Because malignancy of the uterine cervix is typically a disease of young women, we examined the trends in age over the last 4 decades amongst patients with cervical cancer. Starting in the early 1990s, the time at which a significant increase in the proportion of single women with malignancy of the uterine cervix was initially observed, the proportion of women aged <40 years with malignancy of uterine cervix began to decrease significantly (APC, −1.2%; 95% CI=−1.4, −1.0; Fig. 1B). Conversely, the proportion of single women aged ≥40 years has increased over time.
We next examined the effects of age on the trends of single marital status in malignancies of the uterine cervix over the study period. The proportion of older single women (aged ≥40 years) with malignancy of the uterine cervix has increased significantly between 1994 and 2013 (APC, 2.7%; 95% CI=2.3, 3.2; p<0.001). However, no changes were seen in the proportion of affected younger single women (aged <40 years) during this same period (APC, 0.1%; 95% CI=−0.7, 0.6; p=0.850; Fig. 2).
Fig. 2
Temporal trends of single women in malignancy of the uterine cervix stratified by patient age.
Proportions of younger single women (aged <40 years) (yellow line) and older single women among women (aged ≥40 years) (blue line) are shown per calendar year. Dots represent percent and error bar represent 95% confidence interval.
DISCUSSION
Recent United States census data have shown that there is a steady increase in the proportion of single women in the general population during the past 4 decades [1718]. Therefore, our study examined the proportion of single women with malignancies most commonly affecting females. During the study period, the increases in this proportion likely are reflective of the national trends in marital status. An increasing proportion of single women developed various cancers. This would be explained by the increasing age of first marriage and the increase in the number of unmarried women during the study period. In particular, the nearly 5-fold increase in the proportion of single women with malignancy of the uterine cervix during the past 4 decades is noteworthy.
Our study also observed that there was a paradoxical change in the trends of cervical malignancy in single women (increase) and young women (decrease) during the study period, implying that there are now increasing numbers of single women who are older than 40 years with malignancy of the uterine cervix. Indeed, when marital status was stratified by patient age, we found that the proportion of older single women (aged ≥40 years) with cervical malignancy has increased significantly starting around 1990, and this trend was not observed in their younger counterparts (Fig. 2). The decrease in cervical malignancy in the younger population may be partially explained by the higher rate of cervical cancer screening in this group (80%–88%) as compared with the older population (65%) in the United States [19]. In addition, HPV vaccines have been recommended since 2007, and vaccination uptake may contribute to the decrease of malignancy of the uterine cervix in the younger population [2021]. In fact, a previous study has suggested that HPV vaccination is efficacious and safe even in older women [22]. However, older women are unlikely to be covered by insurance for HPV vaccination. Therefore, improving screening and prevention strategies in single women aged ≥40 years would be key to reducing the incidence of cervical malignancy.
Generally, cervical cancer is a highly preventable disease due to effective screening tests and vaccination to prevent infection with high-risk HPV strains. However, disparities in screening compliance exist and may be due in part to perceived barriers or lack of knowledge regarding the risk for cervical malignancy. In fact, cervical cancer screening rates vary across marital status, age, ethnicity, educational qualification, income, and health insurance [19]. Previous data shows that the rate of cervical cancer screening was reported to be lower among single women (78.7%) compared to married women (83.9%) [11]. Since married women have higher rates of pregnancy than unmarried women [23], married women are more likely to undergo gynecologic examinations including performance of the cervical cancer screening. Moreover, married women may have a lower risk of HPV infection than single women due to a consistent sexual partner. This lack of screening, and potential increased exposure to HPV, increases the risk of cervical malignancy. In addition, single marital status was significantly associated with younger age. According to previous studies, single status was associated with poorer prognosis compared to married status [25]. Single marital status is an independent prognostic factor for cervical cancer, therefore suggesting that special consideration for women with single marital status could lead to improved outcomes [5].
The majority of cervical malignancies are seen in women younger than 50 years of age [24]. A bimodal age distribution in HPV prevalence has been previously observed, and the second peak in HPV prevalence in older women is thought to result primarily from persistent infection [25]. It rarely occurs in women greater than 65 years of age who had been previously been screened appropriately. Therefore, multiple societies including American Society for Colposcopy and Cervical Pathology, American Society for Clinical Pathology, American Cancer Society, and the U.S. Preventive Services Task Force published unified cervical cancer screening guidelines, and recommended against screening in women older than 65 years if they have provided adequate prior screening and have no history of moderate- to high-grade dysplasia in the prior 20 years [262728]. More than 15% of cases of cervical cancer are found in women over 65, with the vast majority of these exhibiting infection with multiple genotypes of high-risk HPV [29]. Most older women with high-risk for cervical cancer are not aware that the risk of developing malignancy of the uterine cervix is still present. Therefore, women at older ages reported a reduced utilization of cervical cancer screening [30]. Appropriate screening and education for older single women may contribute to a reduction in cervical cancer rates as well as the associated morbidity and mortality.
The strengths of our study include its population-based design with large sample size. The SEER database represents the largest tumor registry in the United States and is particularly useful for analyzing trends of malignancies among single women, as this requires a large sample size for adequate evaluation. However, the SEER database sample encompasses a relatively small proportion of geographical areas and minority populations, therefore potentially underreporting true incidence. Other limitations of our study include its retrospective design, and possible confounding variables such as missing rates of HPV vaccination and of cervical cancer screening. Other missing confounders include the status for human immunodeficiency virus infection, chronic steroid use, cigarette use, history of metachronous or synchronous cancer, and the explicit reason for the choice of treatment. Additionally, this database is unable to provide information regarding the marital status or the pregnancy history either before or after the diagnosis of the malignancy. These may change throughout the disease course and influence outcomes.
Our findings corroborate other recent studies noting the increased risk of cervical cancer faced by women with single marital status, a characteristic that is not currently taken into consideration in screening guidelines. Clinical implications of our study include potentially re-evaluating current screening and prevention strategies in the target populations of single women, particularly those greater than 40 years of age. Our results identify a subgroup of women at particularly high-risk of malignancy of the uterine cervix who may benefit from additional social support and outreach by the medical community.
 XML Download
XML Download