

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian carcinoma (EOC) has the highest mortality rate among gynecologic malignancies [1]. Early diagnosis of ovarian cancer (OC) is difficult due to the lack of initial symptoms. Thus, OC patients are usually diagnosed at an advanced stage. Nevertheless, approximately 30% of patients present with early-stage disease (International Federation of Gynecology and Obstetrics [FIGO] stages I and II). Such early-stage patients are amenable to complete surgical resection [2]. For patients with stage IA or IB disease and favorable histology, adjuvant therapy is considered unnecessary when thorough surgical staging and histologic confirmation have been performed [3]. In contrast, other patients with early-stage EOC (stage IA or IB and unfavorable histology, including grade 3 or clear cell, stage IC, or stage II) are candidates for adjuvant treatment based upon significant 5-year recurrence rates of 25%–45% [2456].
The optimal adjuvant chemotherapy for high risk group of early-stage EOC patients has been evaluated. Early experience in the Gynecologic Oncology Group (GOG) showed that such patients treated with either intraperitoneal phosphorus-32 or oral melphalan had similar survival rates [37]. Cisplatin in stage IC EOC significantly reduced the relapse rate by 61% [8]. Adjuvant platinum-based chemotherapy is of benefit in early-stage OC [91011]. Cisplatin or carboplatin in combination with paclitaxel has emerged a standard first-line treatment for advanced OC [12131415].
There have been no studies to determine whether or not a platinum plus paclitaxel (PT) regimen yields a better response and outcome than a platinum plus non-paclitaxel regimen in early-stage OC by clinical trials. Besides, there is a debate about the optimal duration of chemotherapy in early-stage EOC. Six cycles of carboplatin and paclitaxel as compared with 3 cycles, did not significantly alter the recurrence rate, but were associated with more toxicity [2]; however, methodologic concerns have led to continued debate about the optimal duration of chemotherapy [1617].
The adjuvant chemotherapeutic regimens of early-stage OC are either platinum plus cyclophosphamide (CP) or PT in Taiwan. The CP regimen could be reimbursed by the national health insurance. Whereas, patients needed to pay by themselves for PT regimen. Given the controversy surrounding the adjuvant chemotherapeutic regimen and number of cycles in patients with early-stage OC, we conducted a population-based analysis to determine if PT regimen yielded better responses and outcomes than a CP regimen. We specifically evaluated adherence to guideline-based recommendations for the administration of adjuvant chemotherapy and analyzed the influence of the duration of chemotherapy on the survival of high-risk patients with early-stage OC.
MATERIALS AND METHODS
1. Study design
This study was approved by the Research Ethics Committee at the National Taiwan University Hospital (NTUH) and is registered in the ClinicalTrials.gov Protocol Registration System (Identifier: NCT01015079). The current retrospective cohort study compared the disease-free survival (DFS) and overall survival (OS) of 2 major regimens of adjuvant chemotherapy after staging surgery of OC patients recommended by the clinical guidelines of gynecologic oncologists in Taiwan, including platinum-analogues combined with cyclophosphamide (CP group) and platinum-analogues combined with paclitaxel (PT group) for 3–6 cycles. The staging surgery included unilateral salpingo-oophorectomy and/or hysterectomy, infracolic omentectomy, and pelvic lymph node sampling or dissection. This study was conducted through computerized linkages with several national databases in the National Health Insurance Research (NHIR) database which contain information regarding demographic characteristics and diagnosis, inpatient and outpatient medical order files, the catastrophic illness registry, and the death certificate registry. The National Health Insurance (NHI) in Taiwan was implemented in 1995 and covers 90%–98% of the population [18] with a comprehensive benefits package, including inpatient and outpatient services. The NHI further provides co-payment reimbursement to patients with catastrophic illnesses, which includes OC. The stages of OC were according to the FIGO staging system [19]. Stages I and II were defined as early stage. Early-stage OC account for 40%–50% of all OC patients, and 65%–70% have received chemotherapy following staging surgery in Taiwan [20]. The NHIR database and this database for cancer with encrypted identification was obtained from and authorized to use by the National Health Research Institutes in Taiwan.
2. Study population
OC patients diagnosed between 1 January 2000 and 31 December 2011 without a history of cancer were identified from the catastrophic illness registry. To identify the patients with early-stage OC (stage I or II), those who underwent debulking surgery (stage III or IV) or staging surgery without adjuvant chemotherapy (stage IA or IB with grade 1), those who received chemotherapy followed by staging or debulking surgery, or those who received paclitaxel-containing regimens reimbursed by the NHI (stage III or IV) were excluded. For a better comparison between the CP and PT groups, those who received the first cycle of chemotherapy >60 days after surgery or the interval of each chemotherapy cycle was >45 days, those who received <3 or >6 cycles of chemotherapy (considered as persistent disease), those who changed the chemotherapeutic regimens within 6 cycles, or those who have undergone radiation after the diagnosis of OC were also excluded from this study. The study flow chart is shown in Fig. 1.
 | Fig. 1Flow chart comparing the chemotherapeutic regimens used for patients with early-stage OC.
CP, platinum plus cyclophosphamide; OC, ovarian cancer; PT, platinum plus paclitaxel.
|
Because the NHI only reimburses platinum analogues combined with cyclophosphamide as adjuvant chemotherapeutic regimens for patients with early-stage OC, those who satisfied the abovementioned criteria and received platinum analogues combined with cyclophosphamide were defined as the CP group. For the PT group, although the NHI did not reimburse paclitaxel, the NHI reimbursed for platinum analogues, H2 blockers, and other anti-histamine-related drugs to prevent adverse effects, such as anaphylactic shock, induced by paclitaxel during a chemotherapy course. It is feasible to retrieve the PT group from the NHIR database when the orders of eligible patients included only platinum analogues as chemotherapeutic drugs with concurrent use of H2 blockers or anti-histamine.
3. Statistical analysis
The frequency of characteristics in the CP and PT groups, including age, wage income, residency, and Charlson co-morbidity index, were retrieved from the NHIR database and compared using a χ2 test to identify possible confounding factors. The number of cycles of the adjuvant chemotherapy course was calculated based on the orders registered in the inpatient and outpatient medical order files. The main outcomes evaluated in this study were recurrence and death. If a new course of chemotherapy at least 1 month after the completion of adjuvant chemotherapy and the following cytotoxic drug, such as paclitaxel, topotecan, liposomal doxorubicin or gemcitabine reimbursed by the NHI, was introduced to the patient, a recurrence was considered to have occurred. The follow-up period for DFS in each patient was calculated from the end of chemotherapy course to the date a new course was initiated. Death ascertainment was retrieved from the death certificate, and the follow-up period for OS was calculated from the end of the chemotherapy course to the date of death. The DFS and OS in different groups were estimated using the Kaplan-Meier method, and the differences in survival curves between the regimens were tested by the log-rank test.
For comparing the effectiveness of CP and PT chemotherapy, hazard ratios (HRs) in different regimens adjusted by confounding factors and the 95% confidence intervals (CIs) were estimated using Cox proportional hazards models.
To assess the degree of overfitting or optimism, a non-parametric bootstrap resampling method was performed by forming 1,000 bootstrap samples of the CP and PT groups of equal size with replacement. Cox proportional regression analyses were estimated and the 95% CIs of the adjusted hazard ratios (aHRs) were calculated. All statistical analyses were performed in SAS version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
1. Characteristics of the patients
A total of 1,510 early-stage OC patients, including 841 who received CP group and 699 who received PT group were included in this study (Fig. 1). The basic characteristics of the 1,510 patients are shown in Table 1. The PT group had a significantly higher insured wage income, urban residence, and received more cycles of chemotherapy than the CP group. The average follow-up period of all patients was 4.60 years (range, 4.46–4.74 years), and 5.17 years for the CP group (range, 4.98–5.37 years) and 3.88 years for the PT group (range, 3.70–4.05 years), respectively.
Table 1
Characteristics of study population by chemotherapeutic regimens
CP, platinum plus cyclophosphamide; NTD, New Taiwan Dollars; PT, platinum plus paclitaxel; SD, standard deviation.
![]()
2. Patients receiving PT regimen had similar DFS and OS compared with patients receiving CP regimen
The DFS and OS of the 1,510 patients analyzed by the Kaplan-Meier method are shown in Fig. 2. The PT group had a similar estimated probability of 5-year (PT vs. CP, 79.0% vs. 77.6%; p=0.410) DFS compared with the CP group (Fig. 2A). The estimated probability of 5-year OS was 84.3% in the CP group and 84.6% in the PT group, respectively (Fig. 2B). The 5-year (p=0.691) OS did not differ significantly between the CP and PT groups, either.
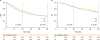 | Fig. 2Survival curves in patients with early-stage OC who received CP or PT chemotherapeutic regimens. (A) DFS (CP vs. PT groups of 2-year DFS: 85.12% vs. 87.59%, p=0.138; 5-year DFS: 77.56% vs. 79.03%, p=0.410) and (B) OS (CP vs. PT groups of 2-year OS: 93.31% vs. 93.81%, p=0.737; 5-year OS: 84.26% vs. 84.56%, p=0.691).
CP, platinum plus cyclophosphamide; DFS, disease-free survival; OC, ovarian cancer; OS, overall survival; PT, platinum plus paclitaxel.
|
3. Different cycle numbers of CP or PT chemotherapeutic regimens had similar DFS and OS
The multivariate Cox model showed that patients receiving 6 cycles of CP, 3–5 cycles of PT, or 6 cycles of PT did not have lower HRs of 2- or 5-year DFS or OS when using 3–5 cycles of CP group as the reference (Table 2). There was no significant difference in the 2- or 5-year DFS or OS between the 4 groups, either.
Table 2
Multivariate Cox model for early-stage OC patients with different chemotherapeutic regimens and number of cycles

aHR, adjusted hazard ratio; CI, confidence interval; CP, platinum plus cyclophosphamide; DFS, disease-free survival; HR, hazard ratio; OC, ovarian cancer; OS, overall survival; PT, platinum plus paclitaxel.
*HR was adjusted for age, insured wage income, residency, and Charlson comorbidity index.
![]()
4. Patients >50 years of age receiving 6 cycles of the PT regimens had significantly longer 2-year DFS than patients receiving 3–5 cycles of the CP regimen
Patients ≤50 years of age had similar HRs in the 5-year DFS or OS, regardless of the number of cycles or chemotherapeutic regimens (Table 3). However, patients >50 years of age receiving 6 cycles of a PT regimen had a significantly lower aHR than patients receiving 3–5 cycles of a CP regimen (aHR=0.53; 95% CI=0.29–0.96; p=0.035) in the 2-year DFS (Table 3).
Table 3
Multivariate Cox model for early-stage OC patients stratified by age group with different chemotherapeutic regimens and number of cycles
HR with p-value <0.05 were in bold face.
aHR, adjusted hazard ratio; CI, confidence interval; CP, platinum plus cyclophosphamide; DFS, disease-free survival; HR, hazard ratio; OC, ovarian cancer; OS, overall survival; PT, platinum plus paclitaxel.
*HR was adjusted for insured wage income, residency, and Charlson comorbidity index.
![]()
5. Patients >50 years of age treated with a CP regimen had a shorter 5-year DFS and OS than the other groups
We first evaluated the 5-year DFS and OS of patients younger and older than 50 years. Patients ≤50 years old had significantly better 5-year DFS (p<0.001; Fig. 3A) and OS (p=0.008; Fig. 3B) than those >50 years old.
 | Fig. 3Survival curves in patients with early-stage OC by age. (A) DFS by age group (≤50 vs. >50 years of 2-year DFS: 88.06% vs. 84.15%, p=0.031; 5-year DFS: 83.48% vs. 71.97%, p<0.001), (B) OS (≤50 vs. >50 years of 2-year OS: 94.71% vs. 92.20%, p=0.053; 5-year OS: 87.06% vs. 81.50%, p=0.008).
DFS, disease-free survival; OC, ovarian cancer; OS, overall survival.
|
The influence of chemotherapeutic regimens was further evaluated. The estimated 2- and 5-year DFS among the 4 groups as a function of age (≤50 or >50 years) and chemo-regimens (CP or PT) were significantly different (p=0.032 for 2 years; p<0.001 for 5 years; Fig. 4A). Patients >50 years of age receiving CP regimens had a lower 5-year DFS than patients ≤50 years of age with CP (p<0.001) or PT regimens (p=0.001). Additionally, patients >50 years of age had a significantly shorter 5-year DFS than patients ≤50 years of age in the CP group (70.49% vs. 83.70%; p<0.001), but not in the PT group (73.35% vs. 82.92%; p=0.063).
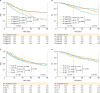 | Fig. 4Survival curves in patients with early-stage OC receiving CP or PT chemotherapeutic regimens grouped by age and number of chemotherapeutic cycles. (A) DFS by age group (5-year DFS: patients ≤50 years of age treated with CP regimen, 83.70%; patients >50 years of age treated with CP regimen,70.49%; patients ≤50 years of age treated with PT regimen, 82.92%;patients >50 years of age treated with PT regimen 73.35%), (B) OS by age group (5-year OS: patients ≤50 years of age treated with CP regimen, 88.26%; patients >50 years of age treated with CP regimen, 79.83%; patients ≤50 years of age treated with PT regimen, 85.29%; patients >50 years of age treated with PT regimen, 83.81%), (C) DFS by number of chemotherapy cycles in all of the patients with early-stage OC (5-year DFS: 3–5 cycles of CP [78.36%], 6 cycles of CP [76.99%], 3–5 cycles of PT [80.43%], 6 cycles of PT [78.29%]), and (D) OS by number of chemotherapy cycles in all of the patients with early-stage OC (5-year OS: 3–5 cycles of CP [86.30%], 6 cycles of CP [82.69%], 3–5 cycles of PT [83.30%], 6 cycles of PT [85.18%]).
CP, platinum plus cyclophosphamide; DFS, disease-free survival; OC, ovarian cancer; OS, overall survival; PT, platinum plus paclitaxel.
|
The estimated 5-year OS among the 4 groups categorized by age (≤50 or >50 years) and chemo-regimens (CP or PT) were significantly different (p=0.029; Fig. 4B). Patients >50 years of age who received the CP regimen had the worse 5-year OS compared with the other 3 groups (p=0.179 for patients >50 years of age in the PT group; p=0.002 for patients ≤50 years of age in the CP group; p=0.061 for patients ≤50 years of age in the PT group; Fig. 4B). Additionally, when comparing the 2 age groups, patients >50 years of age had a significantly shorter 5-year OS than those ≤50 years of age in the CP group (79.83% vs. 88.26%; p=0.002), but not in the PT group (83.81% vs. 85.29%; p=0.644). Patients ≤50 years of age had a similar 5-year OS whether treated with the CP or PT regimen (p=0.350). A similar phenomenon was also observed in patients >50 years of age (p=0.179).
6. The outcome of early-stage OC patients treated in different periods was similar
We then evaluated if treatment period would influence the outcome of early stage OC patients. As shown in Supplementary Table 1, patients treated during 2000–2005 had longer 5-year DFS than those treated during 2006–2010. However, the 5-year OS of the patients was no difference between 2000–2005 and 2006–2010.
7. The cycle number of the 2 chemotherapeutic regimens had similar 5-year DFS or OS in patients with early-stage OC
The patients were further divided by age (≤50 vs. >50 years of age) for the following analysis. As shown in Table 3, among patients ≤50 years of age, no significant differences existed in the 2 chemo-regimen groups with respect to 5-year DFS or OS whether 3–5 or 6 chemotherapy cycles were administered. Among patients >50 years of age in the CP group using 3–5 cycles as the reference group, the aHRs for the 5-year DFS (Fig. 4C) or OS (Fig. 4D) were not significantly different in women >50 years of age who received 3–5 or 6 cycles of either chemotherapeutic regimen.
We further performed bootstrapping to determine if the results of DFS and OS in patients who received the 2 chemotherapeutic regimens were reliable. Table 4 shows the 2- and 5-year DFS and OS in patients with early-stage OC treated with 2 different chemotherapeutic regimens before and after bootstrapping. The aHRs of the 2- or 5-year DFS and OS for the patients who received the 2 chemotherapeutic regimens were not different.
Table 4
DFS and OS in early-staged OC patients treated with 2 different chemotherapeutic regimens before and after bootstrapping
p-values are the comparisons of 95% CI between before and after bootstrapping.
aHR, adjusted hazard ratio; CI, confidence interval; CP, platinum plus cyclophosphamide; DFS, disease-free survival; HR, hazard ratio; PT, platinum plus paclitaxel; OC, ovarian cancer; OS, overall survival.
*HR was adjusted for age, insured wage income, residency, and Charlson comorbidity index.
![]()
DISCUSSION
The optimal management of women with early-stage EOC is a matter of controversy. Since the 1980s, cisplatin-based combination therapy has been shown to be more effective than alkylating agents alone [21] or combinations without cisplatin [2223]. Platinum-based adjuvant chemotherapy with PT has become a common chemotherapeutic regimen for patients with all stages of EOC since 1990s. However, there is no universally preferred platinum-based therapy among oncologists treating OC. The patients treated with paclitaxel had similar 5-year DFS and OS compared to patients treated with cyclophosphamide in this survey (Fig. 2) like Garcia-Saenz's results [24].
The number of cycles of adjuvant chemotherapy in patients with early-stage epithelial OC is another controversial issue. GOG 157 data identified subsets of patients who benefit from additional cycles of chemotherapy. Patients with serous tumors had a significantly decreased risk of recurrence with 6 compared to 3 cycles of chemotherapy (HR=0.33); however, grade 3 or 4 neurotoxicity was significantly increased from 2% to 11% in patients treated with 3 and 6 cycles of therapy, respectively [25]. Another GOG phase III trial comparing observation and weekly maintenance low-dose paclitaxel after 3 cycles of carboplatin and paclitaxel in patients with early-stage OC also showed similar 5-year OS; however, the extended weekly paclitaxel group had higher incidences of peripheral neuropathy, infection or fever, and dermatologic events [26]. Older women (≥50 years) who received 6 cycles of platinum and paclitaxel had a significantly lower risk of recurrence than patients who received 3–5 cycles in this survey. The reasons why patients received different cycles (from 3–6) of chemotherapy include the adverse effects, physicians' recommendation, and patients' decision (such as economic issue).
Age of diagnosis is always an important prognostic factor for patients with EOCs. Young age itself is indeed an independent prognostic factor after adjusting for other well-known clinicopathologic prognostic factors for EOCs [27]. Younger patients with EOCs have better survival than older patients, a finding which has been confirmed in several large population-based studies [1282930]. Several possible explanations for the importance of age in EOC patient survival have been proposed, including performance status [31] and increased tolerance to intensive chemotherapeutic regimens [3233]. Dinkelspiel et al. [34] reported that a higher percentage of older women with early-stage EOC did not receive adjuvant chemotherapy or received adjuvant chemotherapy for a short duration (≤3 months) according to the Surveillance, Epidemiology, and End Results (SEER) data [33]. Our survey revealed that the 5-year DFS of young patients (<50 years) did not differ as a function of the chemotherapeutic regimen or number of cycles; however, older patients (≥50 years) who received 3–5 cycles of platinum and cyclophosphamide had a significantly higher risk of recurrence than patients receiving 6 cycles of platinum and paclitaxel. Older patients with EOCs could benefit (i.e., lower the possibility of recurrence) by receiving paclitaxel regimen and additional cycles of chemotherapy. We hypothesized that older patients had different pharmacokinetics between cyclophosphamide and paclitaxel, and more cycles of paclitaxel could have higher possibility to kill more microscopic tumor cells.
Sub-optimal analysis of the survival results of patients with early-stage EOC is due to incomplete surgical staging and failure to identify prognostic factors. Between 20% and 25% of patients with early-stage EOC relapse, even with adjuvant cytotoxic therapy. The European Organisation for Research and Treatment of Cancer investigated the Adjuvant ChemoTherapy In Ovarian Neoplasm (ACTION) trial and identified that the extent of surgical staging may influence survival [11]. Specifically, patients with sub-optimal surgical staging had significantly worse recurrence-free survival and OS without receiving adjuvant chemotherapy [11]. In contrast, among patients with optimal surgical staging, there was no difference in recurrence-free survival or OS, with or without adjuvant chemotherapy [11]. GOG 157 showed that women with serous tumors had a significantly increased risk of recurrence with 3 cycles of chemotherapy [25]. However, Mannel et al. [26] were unable to replicate the difference in patients with serous tumors. The influence of other histologic types (mucinous, endometrioid, or clear cell) in early-stage OC needs further investigation. Indeed, a poor response of clear cell, mucinous, and low-grade tumors to standard carboplatin/paclitaxel therapy has been reported in multiple trials [353637]. Future treatment trials targeting OC patients based on histologic findings are warranted. Recent genomic analyses indicate that histologic features and grade are better differentiators than stage in OCs [383940]. High-grade serous tumors cluster together regardless of stage and appear different than low-grade serous tumors. Clear cell tumors of the ovary cluster with renal and endometrial/clear cell tumors rather than serous tumors of the ovary, thus suggesting a basic biologic difference which may impact response to therapy. It will be of value to determine if genomic analysis can be used to identify high- or low-risk patients with early-stage EOC who should receive adjuvant chemotherapy.
The strengths of the current study include the nationwide, population-based study design, including almost all patients with early-stage OC using the National Insurance System of Taiwan. With long-term follow-up, the survival status of these patients was documented by death certification, thus resulting in a large, reliable study cohort and robust results without potential selection biases. The shortcomings of this study included the lack of information detail regarding cancer staging, histologic type, histologic grade, and treatment-related morbidities which may have influenced the interpretation of the data. Another limitation of our study was a lack of central pathology. The discordance between different pathologists with respect to site of origin or tumor histopathologic type may also have influenced the study results. Based on this nationwide population-based study, however, the large number of patients may still provide useful information. We believe that our findings still provide meaningful insight into the study of patients with early-stage OC with different chemotherapeutic regimens, which in turn warrant further studies.
The target patients in this study were recruited from the NHIR database and are similar to the real-world database. The same recruiting processes were tested in one medical institute (NTUH) as an internal validation. All of the 163 target patients in the NTUH were recruited from the recruiting processes (Supplementary Fig. 1). And there were 213 patients in the NTUH recruited from the NHIR database by recruiting processes (Supplementary Fig. 2). This internal validation demonstrated that the recruiting processes from the NHIR database are reliable.
In conclusion, early-stage OC patients had similar outcome, when receiving chemotherapeutic regimens with or without taxane. Chemotherapeutic regimens with taxane can improve the survival benefit of early-stage OC patients >50 years of age compared to regimens without taxane.
 XML Download
XML Download