

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of cervical cancer remains high in Korea, despite a decreasing trend [1]. Korean screening guidelines for the prevention of cervical cancer call for a conventional Pap smear or liquid-based cytology every 3 years for asymptomatic women; an additional optional human papillomavirus (HPV) test is also recommended [2]. Because primary HPV screening can lower cancer risk compared to conventional cytology-only screening, it has been considered a viable alternative [3]. HPV is the most important factor that induces transformation of cervical epithelial cells into precancerous lesions or cancer [4]. HPV infection status is thus a crucial element in cervical cancer screening. Consequently, the HPV test has emerged as an important screening tool [56].
Many countries have carried out large-scale vaccination projects that have been highly efficient and lifesaving against cervical cancer [57]. Gardasil® is a commonly used quadrivalent vaccine against HPV types 6, 11, 16, and 18; HPV types 6 and 11 are low-risk (LR) genotypes that induce genital warts or condylomas [8]. Gardasil 9, approved by the United States Food and Drug Administration (US FDA) in 2014, provides protection against HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 [9]. The preventive efficacy of the HPV vaccine against infection has been proven in several studies [81011]. However, all high-risk (HR) HPV types that could cause cervical cancer are not fully covered by Gardasil 9, and prevalent HPV types vary among countries [12]. In addition, various HPV types have different HPV-attributable cancer burdens [13].
Although many studies have reported the prevalence of HPV genotypes based on the presence of precancerous lesions and invasive cancer [141516], a reliable, large-population study has not been reported previously. For these reasons, it is very important to investigate HPV prevalence and type distribution according to cytology and age in Korea. We reviewed data from women who visited a large private Korean healthcare company, and, based on these cross-sectional data, evaluated the prevalence of HPV genotypes according to cervical cytology and age.
MATERIALS AND METHODS
1. Study population
A total of 18,170 women aged 17 to 83 years who visited a large private healthcare company consisting of 7 centers nationwide from January 2014 to December 2016 were included in this study. All patients underwent a gynecologic examination that included collection of a cervical sample for HPV DNA genotyping and cervical cytology via a Papanicolaou-stained conventional smear. Abnormal cytology was reported by pathologists according to the 2001 Bethesda system [17]. The samples were classified as: atypical squamous cells of undetermined significance (ASCUS); atypical squamous cells-cannot exclude high-grade squamous intraepithelial neoplasia (ASC-H); low-grade squamous intraepithelial neoplasia (LSIL); high-grade squamous intraepithelial neoplasia (HSIL); atypical glandular cells (AGC); or unsatisfactory.
All specimens and related data were obtained with approval from the Institutional Review Board of Korea University Guro Hospital (KUGH16216-001).
2. HPV DNA testing
HPV genotyping was done via 2 different methods. Between January 2014 and March 2016, 10,839 samples were analyzed with the HPV Liquid Bead Microarray (Osang Healthcare, Anyang, Korea), which detected 32 types of HPV (6, 11, 16, 18, 26, 31, 32, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 55, 56, 58, 59, 62, 66, 68, 69, 70, 73, 81, and 83). Between April and December 2016, 7,331 samples were analyzed with Anyplex™ II HPV 28 (Seegene, Seoul, Korea), which detected 28 types of HPV (6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 66, 68, 69, 70, 73, and 82). We classified HPV into 19 HR HPV strains (HR HPVs; 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 69, 73, and 82) and 9 LR HPV strains (LR HPVs; 6, 11, 40, 42, 43, 44, 54, 61, and 70) [18].
1) HPV Liquid Bead Microarray
The microarray utilized type-specific oligonucleotide probes for 32 genotypes of HPV DNA, and was based on DNA sequences of the viral L1 gene and specific probes coupled to carboxylated beads (Luminex, Austin, TX, USA). Oligonucleotides, carried by each bead, were ultimately mixed and are referred to as the bead mix. Single-strand polymerase chain reaction (PCR) was used to label the complementary sequences of the probe (Invitrogen, Carlsbad, CA, USA). Thirty-five cycles of amplification were followed by a 5-minute denaturation step at 94°C: denaturation for 30 seconds at 94°C, annealing at 58°C for 1 minute and elongation at 72°C for 2 minutes. The hybridization buffer and HPV mix containing beads were affixed to the PCR products. Then, hybridization was carried out and consequently transferred to a filter plate. Beads were analyzed for R-phycoerythrin receptor fluorescence in the Luminex 100 IS system (Luminex).
2) Anyplex™ II HPV 28
We carried out extraction of HPV DNA in accordance with the manufacturer's guidelines. This real-time PCR test detects 28 HPV DNA genotypes using dual priming oligonucleotides (DPO™, Seegene) and a melting curve analysis method of tagging oligonucleotide cleavage and extension (TOCE™, Seegene). TOCE predicted the melting temperature of the Catcher duplex and offered real-time PCR to HPV 28 using a predetermined target sequence. The L1 gene and human β-globin were amplified concurrently and we measured fluorescence continuously with increasing temperature.
3. Statistical analysis
Age data are presented as the mean±standard deviation. The distribution of HPV genotypes was analyzed by Bethesda system-based cervical cytology and age was divided into 5-year groups. For comparing groups, we used the χ2 test or Fisher's exact test. p<0.05 was considered statistically significant. The data were analyzed with SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Baseline characteristics
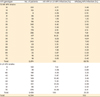
A total 18,170 patients were enrolled with valid results for Anyplex™ II HPV 28 or HPV Liquid Bead microarray cytology. The distributions of age and cervical cytology in patients are presented in Table 1. The mean age was 41.40 years. In terms of cervical cytology, 17,717 women (97.51%) had normal cytology, 228 women (1.25%) had ASCUS, 151 women (0.83%) had LSIL, and 50 women (0.27%) had HSIL/ASC-H. Among the 3,037 (16.7%) women who were positive for HR and/or LR HPV, 2,268 women (12.5%) had HR HPV. Single infections were more common than multiple infections in both the any-HPV genotype group and the HR HPV group.
Table 1
Distribution of age, cervical cytology, and HPV prevalence in enrolled patients (n=18,170)

Values are presented as mean or number (%).
AGC, atypical glandular cells; ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial neoplasia; ASCUS, atypical squamous cells of undetermined significance; HPV, human papillomavirus; HR, high-risk; HSIL, high-grade squamous intraepithelial neoplasia; LR, low-risk; LSIL, low-grade squamous intraepithelial neoplasia.
*HR HPV includes HPV types 6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 66, 68, 69, 70, 73, and 82. LR HPV includes HPV types 6, 11, 40, 42, 43, 44, 54, 61, and 70.
![]()
2. HPV prevalence
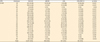
With regard to HPV prevalence, 2,874 HR HPVs and 1,430 LR HPVs were detected in the overall population (Table 2). Among the detected types of HPV, HR HPV 53 was the most frequent type (9.69%), followed by HR HPV 58 (7.90%), HR HPV 52 (7.81%), LR HPV 54 (6.99%), LR HPV 70 (6.41%), HR HPV 16 (5.86%), HR HPV 39 (5.62%), HR HPV 68 (4.93%), HR HPV 51 (4.14%), and HR HPV 56 (4.04%; Fig. 1).
Table 2
Distribution of different detected HPV genotypes
Values are presented as frequencies or percentages.
HPV, human papillomavirus; HR, high-risk; LR, low-risk.
![]()
 | Fig. 1Distribution of HR and LR HPV types among Korean women. HR HPV includes HPV types 6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 66, 68, 69, 70, 73, and 82. LR HPV includes HPV types 6, 11, 40, 42, 43, 44, 54, 61, and 70.
HPV, human papillomavirus; HR, high-risk; LR, low-risk.
|
3. HR HPV positivity by cervical cytology grade
The overall prevalence of the 19 HR HPVs was higher in ASCUS/LSIL cytology than in normal cytology. The prevalence of the 19 HR HPVs increased with increasing cervical cytology severity (p=0.028); HR HPVs were detected in 2,012 (11.4%) of 17,717 cases with normal cytology, 92 (40.4%) of 228 ASCUS cases, 113 (74.8%) of 151 LSIL cases and 45 (90.0%) of 50 HSIL/ASC-H cases (Table 3). However, the risk of multiple infection did not show the same pattern (p=0.211).
Table 3
Positivity for HR HPV by cervical cytology grade

Values are presented as number of cases (%).
ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial neoplasia; ASCUS, atypical squamous cells of undetermined significance; HPV, human papillomavirus; HR, high-risk; HSIL, high-grade squamous intraepithelial neoplasia; LR, low-risk; LSIL, low-grade squamous intraepithelial neoplasia.
*HR HPV includes HPV types 6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 66, 68, 69, 70, 73, and 82.
![]()
4. Prevalence of HR HPV genotypes by cervical cytology
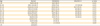
The proportion of HR HPV genotypes detected according to cervical cytology is shown in Table 4. HR HPV 53 was the most frequently detected genotype in normal cytology cases (14.86%). HR HPV 52 (11.63%) and HPV 58 (11.12%) were also common types detected in normal cytology cases. In patients with ASCUS, HR HPV 58 was the most frequent genotype (12.50%), followed by HR HPV 52 (11.90%), HR HPV 53 (8.93%), and HR HPV 16 (7.74%). Similarly, HR HPV 58 was the most frequently detected type in LSIL (13.81%), and the next most frequent types were HR HPV 53 (10.48%), HR HPV 56 (9.52%), and HR HPV 51 (6.67%). The percentage of cases of with HPV 16 detected among the HR HPV genotypes was 24.62%, and was markedly higher in the HSIL/ASC-H group.
Table 4
Prevalence of HR HPV genotypes by cervical cytology
Values are presents as number of patients (%).
ASCUS, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial neoplasia; HPV, human papillomavirus; HR, high-risk; HSIL, high-grade squamous intraepithelial neoplasia; LSIL, low-grade squamous intraepithelial neoplasia.
![]()
5. HPV prevalence in cases with normal cervical cytology and in ASCUS/LSIL cases by age group
HPV prevalence with normal cytology and in ASCUS/LSIL cases is shown stratified by age in Table 5. The rate of 19-HR HPV positivity was 11.4% in the normal cytology group and 54.1% in the ASCUS/LSIL group. Subdivided by age, normal cytology/19 HR HPV-positive results were most common in women younger than 24 years old (32.9%) and decreased with age, and the tendency reached a plateau at 8.9% in women aged 35–39 years. In total, 85.7% of ASCUS/LSIL patients younger than 24 were positive for an HR HPV, while 71.2%, 66.7%, 64.6%, 49.4%, and 22.4% of ASCUS/LSIL patients aged 25–29, 30–35, 35–39, 40–44, or 45–49 years, respectively, were positive for an HR HPV. The prevalence of the 19 HR HPVs increased with age, with 33.3% of women aged 50–54 and 75.0% aged 55–59 testing positive.
Table 5
19 HR HPV positivity with normal cytology and ASCUS/LSIL by age group
Values are presented as number (%).
ASCUS, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial neoplasia; HSIL, high-grade squamous intraepithelial neoplasia; LSIL, low-grade squamous intraepithelial neoplasia.
![]()
DISCUSSION
Among the 18,170 women who enrolled our study, 3,037 (16.7%) were positive for HPV and 2,268 (12.5%) were positive for HR HPV. A notable finding of this study was that HPV 53 was the most common type in Korea and HPV 58, 52, and 16 were also common. Among LR HPV types, HPV 54 and 70 were common. Obviously, HPV positivity was higher in women whose cervical cytology was most advanced (HSIL/ASC-H), higher in LSIL than ASCUS, and higher in ASCUS than in those with normal cytology. Overall and in the normal cytology groups, the most common HPV genotype was HPV 53, whereas HPV 58 was more common in women with ASCUS or LSIL cytology. In addition, HPV 16, widely known to be associated with invasive cervical cancer, was the most common type in HSIL/ASC-H cases [19]. When we classified cervical cytology into normal and ASCUS/LSIL, there was not a significant difference in the prevalence of the 19 HR HPVs among women <59 years old.
In a retrospective worldwide study of HPV-type distribution in invasive cervical cancer, 8,977 of 10,575 patients were positive for HPV. HPV 16 and 18 were the most common types, and those 2 types accounted for 71% of all HPV types detected in invasive cervical cancer [20]. HPV 58 was more frequently detected in Asian cervical cancer cases than in Europe or Africa. Forty-seven years of research on type-specific HPV prevalence among women with invasive cervical cancer in Korea found that HPV 16 (63.1%) was the most prevalent type in invasive cervical cancer, followed by HPV 18 (8.5%), HPV 33 (4.5%), and HPV 58 (3.9%) [21]. Although we did not investigate the prevalence of HPV types in invasive cervical cancer, HPV 16 (24.62%) was the most common type in patients with HSIL/ASC-H, which was the most severe classification in our study. Our findings were consistent with previous research, showing that HPV 16 is most common type in patients with precancerous neoplasia lesions both in Korea [22] and worldwide [142324].
Another Korean study assessed data collected via health check-up from 2008 to 2010 at a single center. Of 7,014 women, 19.7% had HPV, which was higher than our results of 16.7%; however, their reported prevalence of HR HPV (8.4%) was lower than the current study (12.5%) [16]. In that study, the most frequently detected HPV genotypes among all women were HPV 58 (23.9%), HPV 16 (21.8%), HPV 52 (16.6%), and HPV 18 (11.7%), which is discordant with our results. The prevalence of HPV types in their report was 14.51% for HPV 53, 11.83% for HPV 58, 11.69% for HPV 52, and 8.77% for HPV 16, which was somewhat different from our results. However, since their study population had geographical limitations as a single institutional survey of individuals living in an urban setting, the distribution of HPV types in their results are unlikely to reflect national averages. According to recent reports in Korea, HPV prevalence is reported from as low as 16.7% to as high as 40.7% [1625], depending upon the HPV detection method and target population. In particular, the study reporting HPV positivity of 40.7% had the highest prevalence because they targeted commercial sex workers [25]. Although our study population was from a single institution, there were broadly distributed branches nationwide, and so they more accurately represent Korean women in general.
We found that HPV 53 was the most prevalent type in Korea, which was inconsistent with previous Korean studies, [162225262728] with one exception; So et al. [22] reported that the most common HPV type in Korea was HPV 53. Because we analyzed patients who visited 7 centers of Korea Medical Institute (KMI) nationwide in Korea, our results could more closely mirror the general population. In addition, our data were more recent, from January 2014 to December 2016, and the only large-population study in Korea to date, and so the results could be interpreted as indicating that the incidence of HPV 53 has increased over time. Unfortunately, although HPV 53 was the most frequent HPV type in our data, it is not an HPV genotype that Gardasil 9 targets. Nonetheless, HPV 53-related cervical cancer is very rare, not only in Korea, but also internationally [202729].
This study has several limitations. First, we enrolled women who underwent health examinations at KMI, which was a private corporation. These results may not reflect the general population of Korea, since women who participated in our study were volunteers who were screened at KMI. Due to the small number of volunteers aged >50, the results may not be accurate for this age group. Furthermore, numerous women avoid HPV tests or Pap smears because of a fear of pelvic examinations [30]. Second, we could not access information on whether participants were vaccinated. However, it was important to analyze the present prevalence of HPV, so we focused on the standard HPV prevalence data for Korea. Lastly, HPV DNA testing was carried out using 2 different systems, the HPV Liquid Bead Microarray and Anyplex™ II HPV 28. Although both detection systems have been validated, [3132] using 2 systems might be less accurate than using just one HPV genotyping method.
In conclusion, we described the prevalence and distribution of HPV genotypes by age and cytology for 18,170 women who voluntarily visited a healthcare institute. Knowledge of epidemiologic HPV genotypes will be helpful for creating effective HPV screening strategies and developing targeted, protective HPV vaccines. Furthermore, our study of HPV genotypes in Korea provides important baseline data for evaluating the effectiveness of the newly implemented National Immunization Program (NIP) HPV vaccine program. Further studies of changes in the prevalence and distribution of HPV genotypes after implementation of the NIP are needed.
 XML Download
XML Download