

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Globally, cervical cancer remains the most common gynecologic malignancy [1]. In Japan, nearly 80% of women with cervical cancer are diagnosed with either stage I (up to 50%) or stage II (up to 25%) disease [2]. In Japan, women with these early-stage cervical cancers typically undergo surgical treatment with radical hysterectomy and pelvic lymphadenectomy [2]; however, the current evidence-based guidelines per the Japan Society of Gynecologic Oncology (JSGO) are lacking in specific indications for para-aortic lymph node (PAN) dissection at the time of surgical treatment [3]. Similarly, the National Comprehensive Cancer Network (NCCN) guidelines for cervical cancer in the United States indicate that PAN sampling is optional without specifying concrete recommendations for PAN dissection at the time of radical hysterectomy for stage IB cervical cancer [4].
In a view of current practice pattern for surgical treatment for women with early-stage cervical cancer in Japan, nearly two thirds of the Japanese Gynecologic Oncology Group (JGOG) designated institutions perform additional PAN dissection during radical hysterectomy for stage IB–IIB cervical cancer [5]. The indications for PAN dissection vary across the institutions making it difficult to assess the true benefits and risks related to PAN dissection [5]: common indications for PAN dissection include histologic evidence of common iliac or pelvic lymph node (PLN) metastasis, radiographic or clinical suspicions for PAN metastasis, cancer stage, and histology type. Moreover, the extent of PAN dissection seems to vary among the institutions in Japan, and routine PAN dissection to the level of infra-renal vessels is rarely performed even though nearly one third of PAN metastasis can be seen in the infra-renal nodal chain without infra-mesenteric artery chain metastasis [6].
Because PAN metastasis is not an uncommon clinical entity in early-stage cervical cancer [78], identification of PAN metastasis is crucial in its management, as it impacts not only patient prognosis but also the surgical approach and choice for adjuvant therapy after surgery [89]. The objective of the study was to examine the surgical-pathological factors related to PAN metastasis at radical hysterectomy, and to identify predictors for PAN recurrence among women who did not undergo PAN dissection at radical hysterectomy.
MATERIALS AND METHODS
1. Eligibility
We retrospectively analyzed the previously organized nation-wide large-scale observational cohort study that was conducted in 116 JGOG participating institutions [10111213]. In this study, consecutive cases of women with stage IB–IIB cervical cancer who underwent a radical hysterectomy between January 1, 2004 and December 31, 2008 were collected with the data acquisition time period being between October 1, 2012 and February 28, 2013.
Women with stage IB–IIB cervical cancer who underwent a type III radical hysterectomy with available results for PAN status were eligible for this study, while those with unknown PAN status were excluded. Institutional Review Board (IRB) approval was obtained at Tottori University (the host institution, IRB registration No. 2129) and the JGOG-participating institutions reviewed the protocol and obtained IRB approval as indicated. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for the retrospective observational studies to outline this study contents and results [14].
2. Clinical information
Clinico-pathological variables recorded in the database were patient age at surgery, histologic subtype, clinical cancer stage, pathological cancer stage, tumor size, parametrial tumor involvement, deep cervical stromal tumor invasion, lympho-vascular space invasion (LVSI), uterine corpus tumor involvement, malignant cells in peritoneal cytology, ovarian tumor involvement, and lymphadenectomy status (PLN and PAN). In each nodal site, the number of sampled lymph nodes and number of tumor-involved lymph nodes were abstracted. For PAN status, women who did not undergo PAN dissection due to no suspicion of PAN metastasis based on clinical, radiographic, and intraoperative assessment were recorded as clinically PAN-negative cases. Multiple PLN was defined as the presence of 2 or more tumor-involved lymph nodes.
Recorded postoperative adjuvant therapy was grouped into: whole pelvic radiotherapy-based, systemic chemotherapy alone, or no adjuvant therapy. Among women who received radiotherapy, the use of additional aortic-boost radiation was abstracted. Additionally, the anatomical location of the first recurrence was abstracted among women who developed recurrent disease. For this study, specific anatomical sites for PAN recurrence were examined, and time to PAN recurrence was determined from the date of surgery to the date of the PAN recurrence. In our practice PAN recurrence is generally made by radiographic assessment with or without histological assessment. The patients who did not develop PAN recurrence were censored.
3. Statistical analysis
The primary interest of this analysis was to examine independent predictors for PAN metastasis at the time of radical hysterectomy (PAN metastasis cohort). The secondary interest of analysis was to determine independent predictors for PAN recurrence among women who were clinically PAN-negative and did not undergo PAN dissection at radical hysterectomy (PAN recurrence cohort). In each cohort, combination patterns of independent risk factors for PAN metastasis/recurrence were assessed, and incidence risks were determined in each risk combination pattern.
Continuous variables were assessed for normality with the Kolmogorov-Smirnov test expressed with mean (±standard deviation) or median (interquartile range). The statistical significance of continuous variables was assessed with Student's t-test or Mann-Whitney U test, as appropriate. Categorical or ordinal variable were assessed with Fisher exact or χ2 test as appropriate.
In an analysis of the PAN metastasis cohort, a binary logistic regression model was used to determine the independent risk factors for PAN metastasis. In this model, all the significant covariates in univariate analysis were entered in the final model. The magnitude of statistical significance was expressed with adjusted odds ratio (aOR) with 95% confidence interval (CI). The Hosmer-Lemeshow test was used to assess the goodness-of-fit of the model, and p>0.05 was interpreted as a good model. In addition, we performed a sensitivity analysis to examine predictors for PAN metastasis in a group of women who had PAN dissection and in a group of women who did not receive neoadjuvant chemotherapy.
In an analysis of PAN recurrence after the initial surgical treatment, a time-dependent analysis was utilized because recurrence of disease is an event over follow-up course. The Kaplan-Meier method was used to construct cumulative incidence curves, and statistical significance between these curves was determined by the log-rank test. Cox proportional hazard regression models were used to assess the independent predictors for PAN recurrence among women with clinically PAN-negative at radical hysterectomy. All the significant covariates on univariate analysis were entered in the final model, and the magnitude of statistical significance was expressed with an adjusted hazard ratio (aHR) and 95% CI.
Over-fitting in the multivariate model was assessed with ratio of event per the covariates entered in the final model, and ratio <10 were interpreted as over-fitting. All statistical analyses were based on 2-side hypothesis, and a p-value of less than 0.05 was considered significant. Statistical Package for Social Sciences (SPSS) version 24.0 (IBM Corp., Armonk, NY, USA) was used for the analysis.
RESULTS
1. Study population
Patient selection schema of the study is shown in Fig. 1. Among 6,003 cases in the database for the JGOG-1072S study, we excluded 39 cases in which surgery was performed outside the study period and 344 cases in which information for PAN was not available. The remaining 5,620 women with stage IB–IIB cervical cancer who underwent radical hysterectomy with available PAN status represented the study population. These included 957 (17.0%) women who underwent surgical PAN dissection and 4,663 (83.0%) women who did not undergo surgical PAN dissection due to lack of clinical suspicion for PAN metastasis.
 | Fig. 1Study selection schema. Green box indicates the independent risk factors for PAN metastasis at the time of radical hysterectomy (left box), and independent predictors for PAN recurrence for clinically PAN-negative cases at radical hysterectomy (right box). Common surgical-pathological factors are emboldened.
CxCA, cervical cancer; JGOG, Japanese Gynecologic Oncology Group; LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; RH, radical hysterectomy.
|
2. Risk factors for PAN metastasis at radical hysterectomy
Among 5,620 women who underwent radical hysterectomy, there were 120 (2.1%; 95% CI=1.8–2.5) women who had PAN metastasis. Patient demographics of women who had PAN metastasis are shown in Table 1. Higher clinical stage, large tumor, parametrial involvement, deep stromal invasion, LVSI, uterine corpus invasion, malignant peritoneal cytology, and PLN metastasis were significantly associated with increased risk of PAN metastasis on univariate analysis (all, p<0.001). For the extent of PAN dissection, women with PAN metastasis were more likely to have higher PAN counts compared to those without PAN metastasis (median, 13 vs. 8 sampled lymph node counts; p<0.001).
Table 1
Surgical-pathological factors based on PAN metastasis (n=5,620)

Data shown are number (%) per row, mean (±standard deviation), or median (interquartile range). Student's t-test, Mann-Whitney U test, or χ2 test for p-values. Significant p-values were emboldened.
Adeno, adenocarcinoma; AS, adenosquamous; LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; PLN, pelvic lymph node; SCC, squamous cell carcinoma.
![]()
Independent predictors for PAN metastasis at radical hysterectomy were examined (Table 2). On multivariate analysis, parametrial involvement (aOR=1.65), deep cervical stromal invasion (aOR=2.61), ovarian metastasis (aOR=3.10), and pelvic nodal metastasis (single-node aOR=5.39 and multiple-node aOR=33.5, respectively) remained independent risk factors of PAN metastasis (all, p<0.05).
Table 2
Independent risk factors for PAN metastasis

A multivariate logistic regression model for PAN metastasis. Significant covariates on univariate analysis were entered in the final model. Significant p-values were emboldened. Clinical stage was not entered due to multicollinearity. Hosmer-Lemeshow test p=0.74, indicating goodness-of-fit in the final model.
aOR, adjusted odds ratio; CI, confidence interval; LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; PLN, pelvic lymph node.
![]()
The incidence of PAN metastasis was examined based on the combination patterns of independent risk factors. A total of 20 combination patterns were identified (Table 3). There were 2,044 women who had no risk factor, and with absence of these four factors, the incidence of PAN metastasis was less than 1% (0.9%). Conversely, more than 20% of the study population (n=1,151, 22.5%) had a risk factor patterns placing them at a ≥4% risk of PAN metastasis (9 risk factor patterns as embolden in Table 3). Of those, more than half of these combination patterns had deep cervical stromal invasion (7 patterns) or multiple PLN metastasis (5 patterns).
Table 3
Risk factor-based incidence of PAN metastasis
Data shown are number (%). Among 5,098 cases with available results for these four risk factors, incidence of PAN metastasis was examined based on patterns of risk factors. Patterns wit risk of PAN metastasis ≥4% are emboldened.
PAN, para-aortic lymph node; PLN, pelvic lymph node.
![]()
In a sensitivity analysis, predictors for PAN metastasis were examined in 957 women who had histological PAN evaluation (Supplementary Tables 1 and 2). Results were similar to the whole cohort in that parametrial involvement (aOR=1.90) and PLN metastasis (single-node aOR=4.99 and multiple-node aOR=28.1, respectively) were independently associated with PAN metastasis (both, p<0.05). Both deep cervical stromal invasion (aOR=2.36; p=0.08) and ovarian metastasis (aOR=2.23; p=0.16) pointed towards increased risk of PAN metastasis but did not reach statistical significance.
In a separate sensitivity analysis, we examined risk factors for PAN metastasis among 4,547 women who underwent primary radical hysterectomy without neoadjuvant chemotherapy (Supplementary Tables 3 and 4). In this group, there were 87 women (1.9%; 95% CI=1.5–2.3) who had a PAN metastasis. On multivariate analysis, ovarian metastasis (aOR=4.08) and PLN metastasis (single-node aOR=7.87 and multiple-node aOR=51.0, respectively) remained independent predictors for PAN metastasis at surgery (both, p<0.05).
3. Predictors for PAN recurrence among clinically PAN-negative women
Among 4,663 women who did not undergo PAN dissection at the time of radical hysterectomy due to an impression of no PAN metastasis, there were 195 (4.2%) women who developed PAN recurrence during the postoperative follow-up course (Fig. 1). The median follow-up time among cases without PAN recurrence was 62.2 months. The median time to develop PAN recurrence was 16.1 months. The PAN recurrent risk in clinically PAN-negative cases was significantly higher than the histologically PAN-negative cases (4.2% vs. 2.5%; aHR=1.60; 95% CI=1.01–2.54; p=0.046). In the histologically PAN-negative group, the median time to develop PAN recurrence was similar to the clinically PAN-negative group (16.2 months). The PAN recurrence risk was exceedingly high in women with histologically PAN metastasis (22.5%) with a median time to develop PAN recurrence of 10.8 months.
Patient demographics for women who developed PAN recurrence are shown in Table 4. On univariate analysis, tumor factors related to PAN recurrence were histology, higher clinical stage, large tumor size, parametrial involvement, deep cervical stromal invasion, LVSI, uterine corpus invasion, malignant peritoneal cytology, ovarian metastasis, and PLN metastasis (all, p<0.05). On multivariate analysis (Table 5), large tumor size (aHR=1.48), parametrial involvement (aHR=1.63), LVSI (aHR=1.74), ovarian metastasis (aHR=3.05), and PLN (single-node aHR=2.47 and multiple-node aHR=8.34, respectively) were independently associated with PAN recurrence (all, p<0.05).
Table 4
Surgical-pathological factors for the clinically node-negative cohort based recurrence pattern (n=4,663)

There were 3 cases with no information for recurrence. Data show number (%) per row, mean (±standard deviation), or median (interquartile range) are shown. Student's t-test, Mann-Whitney U test, or χ2 test for p-values. Significant p-values were emboldened.
Adeno, adenocarcinoma; AS, adenosquamous; LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; PLN, pelvic lymph node; SCC, squamous cell carcinoma.
![]()
Table 5
Independent risk factors for PAN recurrence

A Cox proportional hazard regression model for multivariate analysis. All the listed covariates were entered in the final model. Significant p-values were emboldened.
aHR, adjusted hazard ratio, CI, confidence interval; LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; PLN, pelvic lymph node; RT, whole pelvic radiotherapy; SCC, squamous cell carcinoma.
![]()
Cumulative PAN recurrence was evaluated based on the combination patterns of independent risk factors (Table 6). A total of 19 combination patterns were identified. There were 1,769 women who had no risk factor, and with absence of these four factors, a 5-year cumulative PAN recurrence risk was less than 1% (0.8%). Conversely, more than 15% of this study population (n=706, 16.3%) had a risk factor patterns placing them at a 5-year PAN recurrence risk of ≥8% (8 risk factor patterns as embolden in Table 6). Of those 8 risk factor patterns, the vast majority of risk-combination patterns were related to lymphatic spread (6 patterns for LVSI, and 6 patterns for multiple PLN metastases).
Table 6
Recurrence risk at PANs based on risk factor pattern among clinically negative PAN at radical hysterectomy
Among 4,325 cases with complete information for the five risk factors, cumulative recurrence risk to PAN was examined based on the patterns of risk factors. Patterns with risk of PAN recurrence ≥8% are emboldened.
LVSI, lympho-vascular space invasion; PAN, para-aortic lymph node; PLN, pelvic lymph node.
*Five-year cumulative recurrence risk of PAN recurrence.
![]()
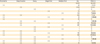
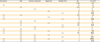
In an exploratory analysis, we examined the effectiveness of para-aortic boost radiotherapy among those who received postoperative radiotherapy. Among women who had PLN metastasis but did not undergo PAN dissection at radical hysterectomy, para-aortic boost radiotherapy was associated with lower PAN recurrence risk although it did not reach statistical significance: single PLN metastasis (5-year cumulative risk for boost vs. non-boost, 0% vs. 5.2%; p=0.48) and multiple PLN metastases (12.0% vs. 20.3%; p=0.23; Fig. 2A). Among 120 women who had a PAN metastasis at radical hysterectomy, aortic boost radiotherapy was associated with decreased risk of PAN recurrence but did not reach statistical significance (15.3% vs. 32.6%; p=0.09; Fig. 2B).
 | Fig. 2Cumulative risk of PAN recurrence. Log-rank test for p-values. Cumulative incidence of PAN recurrence is shown for (A) multiple PLN metastases cases without PAN dissection at radical hysterectomy, and (B) PAN metastasis cases at radical hysterectomy.
PAN, para-aortic lymph node; PLN, pelvic lymph node.
|
DISCUSSION
In this study, parametrial tumor involvement, ovarian metastasis, and PLN metastasis particularly with multiple nodal involvement, are 3 surgical-pathological risk factors commonly seen in the PAN metastasis cohort and the PAN recurrence cohort. They are biologically plausible risk factors for increased risk of tumor spread to para-aortic lymph nodal chain in cervical cancer by 2 routes: 1) lymphatic spread via ovarian drainage; and 2) lymphatic spread via pelvic nodal drainage (Fig. 1).
Anatomically, the ovary is in greatest proximity to PAN compared to other reproductive organs including the uterus and the cervix. Therefore, when the ovary harbors the tumor of cervix, there is a greater chance of spread to PAN via the lymphatic route through gonadal vessels as compared to spread from other organ sites. Patterns of tumor spread from the uterine cervix to the ovary are likely either lymphatically or hematogenous through the uterine vessels [1516]. In addition, close anatomical spread from the uterine corpus to the ovary can occur [1718]. While ovarian metastasis in cervical cancer is relatively rare [1116], it is significantly associated with decreased survival [11]. In our study, ovarian metastasis represents the second most significant factors for PAN metastasis and recurrence. Therefore, if ovarian metastasis is preoperatively suspected and intraoperatively confirmed, systematic PAN dissection would be highly recommended.
This study also suggests a pattern of PAN metastasis via parametrial tumor spread to PLN and supports others who have proposed this pattern [19]. Tumors with deep cervical stromal invasion and LVSI increase the risk of PLN metastasis; and bilateral PLN metastases further increase the risk of PAN [19]. In our study, deep cervical stromal invasion and parametrial tumor involvement, two findings that are representative of aggressiveness of local tumor spread, were independently associated with an increased risk of PAN metastasis (Table 2). LVSI was also independently associated with PAN recurrence among clinically PAN-negative women (Table 5). Most importantly, a finding of multiple PLN metastases was strikingly associated with increased risks of both PAN metastasis and recurrence, holding the largest magnitude of statistical significance among independent predictors for PAN metastasis/recurrence. Therefore, when multiple PLN metastases are identified intra-operatively, common iliac lymphadenectomy alone would not be sufficient and a thorough PAN dissection is highly recommended [20].
The PAN recurrence rates of 2.5% to 4.2% in clinically/histologically PAN-negative cases in our study are similar to what has been reported in the literature (1.4%–3.5% for stage I–II disease) [21]. However, PAN recurrence rate of 22.5% among women who had a PAN metastasis at the time of radical hysterectomy is concerning. In this group, there was a trend of decreased PAN recurrence with postoperative aortic boost radiotherapy (15.3%), and the PAN recurrence rate was extraordinarily high without aortic boost radiotherapy (32.6%). These results imply that a thorough and complete PAN dissection alone for women with known PAN metastasis may not have a therapeutic implication to reduce PAN recurrence. Moreover, extensive PAN dissection for known PAN metastasis case may not be optimal when considering the high recurrence risk and the intra- or post-operative surgical morbidity from the procedure. While limited PAN resection for macroscopic lesions followed by aortic boost radiotherapy in known PAN metastatic cases can be considered as an approach, the benefit of this strategy was not able to be demonstrated using the variables available in this database.
The utility of our study results can be applicable towards the intra-operative assessment for PAN metastasis. We identified four independent predictors for PAN metastasis at surgery (Fig. 1). These include parametrial tumor involvement, deep cervical stromal invasion, ovarian metastasis, and PLN metastasis. These four factors can be evaluated intra-operatively via gross assessment (macroscopic) and/or frozen section of the specimen (microscopic). The incidence table provided in this study (Tables 3 and 6), then, can guide the risk of PAN metastasis to aid in assessment of the need for PAN dissection during radical hysterectomy. Although not ideal, in institutions lacking infrastructure support or manpower for intra-operative frozen section, pre-operative imaging assessment would be valuable in preoperative assessment in the need for PAN dissection. Uterine corpus invasion can be a surrogate marker for ovarian metastasis, and preoperative magnetic resonance imaging (MRI) can be useful to evaluate the uterine corpus tumor invasion [22].
The 2 possible anatomic routes of spread to PAN can be used to guide surgical management. That is, patterns of PAN spread either via the ovarian/uterine corpus route or the pelvic route through pelvic/parametrial lymphatic chain can impact the extent of PAN dissection at the time of surgery. First, if the ovarian/uterine corpus route of spread is involved, it may be more appropriate to perform PAN dissection in the area of high-aortic nodal bundle (infra-renal vessel chain) rather than the low-aortic nodal bundle (infra-mesenteric artery chain), as this is where gonadal vessels drain into the vena cava or aortic systems. On the contrary, if the pelvic route is involved with the tumor, the tumor will likely spread primarily to the low-aortic nodal bundle instead of the high-aortic nodal bundle. Therefore, in such cases, it is necessary to proceed with PAN dissection at the low-aortic nodal bundle first. If the low-aortic nodal bundle is involved with the tumor, then additional PAN dissection in the area of the high-aortic nodal bundle would be reasonable.
Strengths of the study are that the sample size is one of the largest in the literature, and that 2 sets of a cohort within the dataset demonstrated the consistency for risk factors for PAN metastasis/recurrence and serve as internal validation. We also noticed multiple limitations and weaknesses in the study. First, this is a retrospective study that may miss confounding factors. For example, the indication and anatomical extent of PAN dissection was not abstracted in the study. Therefore, we do not know what proportion of the case received PAN to the level of infra-renal vessels. In addition, we do not know if ovarian metastasis assessment was based on macroscopic or microscopic findings. More importantly, we do not have information regarding intra- and post-operative complications related to PAN dissection and aortic boost radiotherapy. This information would be particularly important to weigh risk-benefit ratios for PAN dissection.
Currently, the JSGO guidelines only indicates that PAN dissection is recommended when there is a high suspicion for PAN metastasis [2]; however, this is not based on thoroughly evaluated evidence, and moreover, there is no objective schema or triage system guiding performance of PAN dissection at the time of radical hysterectomy. In this study, we provided a concrete incidence list for PAN metastasis and recurrence that can be integrated into practice patterns. The threshold to perform PAN dissection is yet determined in this study, and we used arbitrary cutoffs of 4% for PAN metastasis and 8% for PAN recurrence based on clinically meaningful significance compared to overall PAN metastasis/recurrence found in our study (PAN metastasis up to 2%, and PAN recurrence up to 4%). Indeed, we found that a significant proportion (nearly 1 in 5) of women with stage IB–IIB cervical cancer was at-risk population of PAN metastasis. Further cost-effective studies would be necessary to determine the ultimate cutoff value to intervene PAN dissection.
 XML Download
XML Download