

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the fifth leading cause of cancer death among women in the United States and has the highest mortality rate of all gynecologic cancers [1]. In 2014, approximately 21,980 new cases of ovarian cancer were diagnosed in the United States, and 14,270 women died of the disease [1]. Although 90% of ovarian cancers are epithelial in origin, the remaining 10% comprise germ cell tumors, sex cord stromal tumors, soft tissue tumors not specific to the ovary, unclassified tumors, and metastatic tumors.
Teratomas, a type of germ cell tumor, may be composed of mature or immature tissues derived from the 3 germ cell layers [23]. More than 80% of mature cystic teratomas (MCTs) develop during the reproductive years [4]. MCTs represent 62% of all ovarian neoplasms in women younger than 40 years [5]. More than 80% of malignant transformations (MTs) of teratomas are to squamous cell carcinomas (SCCs) arising from the ectoderm; the remaining MTs are to carcinoid tumors or adenocarcinomas [67]. Prolonged exposure to various carcinogens in the female pelvic cavity might cause a malignant change in MCTs [8]. Furthermore, high-risk human papillomavirus (HPV) infection might be associated with ovarian SCC [91011].
It accounts for 1.5%–2.3% of all primary ovarian malignant tumors [6]. The prognosis of these malignancies is poor [12]. However, the clinicopathologic characteristics, treatment, and prognostic factors are not yet well understood because of the rarity of these tumors. The use of imaging techniques, such as gynecological sonography, computed tomography (CT), and magnetic resonance imaging (MRI), for detecting calcified tissues, namely teeth, bone, and cartilage, in tumors makes it easy to diagnose MCTs preoperatively [1314]. Therefore, the early detection of MT to SCC is essential in clinical practice. However, the MT of MCTs is very difficult to diagnose pre- or intraoperatively. Thus, it is crucial to determine the clinicopathologic characteristics of MT of MCT to SCC. Accordingly, we analyzed the records of patients from multiple medical centers in Taiwan who developed these rare tumors, and we reviewed related literature.
MATERIALS AND METHODS
This is a cooperative study conducted across multiple medical centers by the Taiwanese Gynecologic Oncology Group (TGOG) after approval from the institutional review board. Pathological reports of 16,001 patients with primary ovarian cancer who were treated at 10 Taiwan medical centers from 1990 to 2011 were reviewed. Malignant cases with incidental MCT unrelated to SCC MT were excluded.
In total, 52 patients with MT of MCT to SCC were identified. Data on demographics, presenting symptoms, preoperative evaluation, surgical management, pathological findings, adjuvant therapy, follow-up, and treatment outcomes were obtained from the medical records. Surgical staging in most cases included hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic and para-aortic lymphadenectomy. Surgical stage was reported using the 1988 International Federation of Gynecology and Obstetrics (FIGO) staging system. Multiple variables were examined including age, surgical stage, grading, tumor size, tumor markers, adjuvant chemotherapy/radiotherapy/concurrent radiotherapy, and whether or not there was death secondary to disease. Survival time was measured as time from the initial diagnosis to the time of death or last contact. The statistical analysis was conducted with SPSS software (IBM Corp., Armonk, NY, USA). p<0.05 was considered as significance. Survival curves were analyzed using the Kaplan-Meier method, and the differences in survival were assessed using the log-rank test.
RESULTS
According to the computerized database and cancer registry of multiple centers, 24,040 patients with ovarian MCT and 16,001 patients with primary ovarian cancer underwent surgery during the study period. According to the pathological reports of these patients, 52 showed MT of MCT to SCC. The characteristics of these 52 patients are summarized in Table 1.
Table 1
Patients and tumor characteristics (n=52)
1. Age at diagnosis
The median and mean ages of the 52 patients were 52 years (range, 29–89 years) and 52.1 years, respectively. Among them, 27 (51.9%) and 25 (48.1%) patients were postmenopausal and premenopausal women, respectively.
2. Presenting symptoms
All patients presented with more than one symptom related to the tumor. The most common presenting symptoms were a palpable abdominal mass, abdominal distension, and lower abdominal pain. Other minor symptoms included voiding difficulty, low back pain, and weight loss. One patient exhibited preoperative cyst rupture.
3. Results of preoperative evaluation
All patients underwent preoperative imaging: gynecological ultrasonography (n=34), abdominal and pelvic CT (n=25), and abdominal and pelvic MRI (n=5). The median tumor size was 10.8 cm (range, 1–40 cm). In our one of case, an abdominal CT scan revealed a huge cystic mass (18 cm), mainly in the lower abdomen, and presented with several enhanced, irregular, and solid components. The tumor margin was ruptured at one enhanced solid component (Fig. 1A), and the abdomen was filled with moderate amounts of ascites with thickened, well-enhanced peritoneum.
Fig. 1
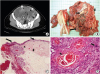
(A) malignant teratoma with rupture in a 36-year-old woman. Post-contrast abdominal CT scan showing well circumscribed mass occupying pelvis, having enhancing solid soft tissue (arrow), fat component (arrow head) and calcifications (dashed circle). (B) Tumors were predominantly cystic, filled with pultaceous material and hair (long arrow) and teeth (middle arrow). Foci of solid areas were also identified (short arrow). (C) SCC MT from MCT. Cystic tumor consists of 3 germ cell components: ectoderm-squamous cell epithelium (middle long arrow), mesoderm-adipose tissue (short arrow), sebaceous gland (arrowhead), endoderm-pseudostratified columnar epithelium (long long arrow). (D) SCC MT from the MCT with hyperchromatic and pleomorphic nuclei (long arrow) and keratin pearl formation (short arrow) (H&E, ×400).
CT, computed tomography; H&E, hematoxylin and eosin; MCT, mature cystic teratoma; MT, malignant transformation; SCC, squamous cell carcinoma.
4. Surgical management
All patients underwent primary surgical treatment. Two patients, who were referred from other hospitals for further management after incomplete surgery, underwent secondary surgical management for restaging. A total of 33 (63%) patients underwent the complete staging procedure, including lymphadenectomy, omentectomy, and appendectomy. Eighteen patients developed ascites; fluid collection was >100 and >1,000 mL in 10 and 5 patients, respectively. The FIGO stages were as follows: IA (n=18), IB (n=1), IC (n=7), IIB (n=3), IIC (n=3), IIIC (n=10), IV (n=3), and unknown stage (n=7). Among the 18 stage IA patients, 9 (50%) did not undergo the complete staging procedure.
5. Pathological findings
All tumors with MT to SCC contained various amounts of hair with greasy and sebaceous liquid, cartilage, and/or teeth as shown in Fig. 1B-D.
6. Adjuvant therapies
The application of adjuvant therapy in patients was as follows: 10 of 26 stage I, 4 of 6 stage II, and 9 of 10 stage III patients received adjuvant chemotherapy; 6 received concurrent chemoradiotherapy (CCRT); 3 received radiation therapy (RT); and one received RT and CCRT. Platinum-based combination chemotherapeutic regimens were mostly used. The mean number of chemotherapy cycles was 5 (range, 2–9).
7. Prognosis categorized by FIGO age, stage, and treatment modality
On the basis of clinical data such as age, FIGO stage, adjuvant treatment modality, follow-up period, and status at last follow-up, we analyzed the prognosis of SCCs arising from MCTs. According to our data, there were no statistical differences in the survival times of patients classified by age as continuous variable. Among the 52 SCC patients, 7 did not have a documented FIGO stage, and 11 patients were excluded because their follow-up data were unavailable. Accordingly, 41 patients were included in the analysis. The median follow-up period was 89 weeks (range, 1–1,100 weeks). Overall patient survival categorized by FIGO stage is shown in Fig. 2A. Patients with tumors that spread beyond the ovary (FIGO stages II–IV) had a very low probability of long-term survival. The 5-year survival rate for stage I patients was 93%, indicating that the early detection of MT before the occurrence of invasion or metastasis is essential for treating SCC. Fig. 2B describes the overall survival according to the adjuvant treatment modality applied in patients with tumors that spread beyond the ovary (FIGO stages II–IV). The survival times were longer in patients who received adjuvant chemotherapy or CCRT than in those who received adjuvant RT alone or no adjuvant therapy at all, indicating that chemotherapy or CCRT may have a role in treating SCC (Fig. 3A).
Fig. 2
(A) The median follow-up time was 89 weeks (range, 1–1,100 weeks). Overall survival by FIGO stage is shown. Five-year survival rate for patients with FIGO stage I disease was 93%. (B) Patients with FIGO stages II–IV had low probability of long-term survival, comparing to patients with stage I disease (p<0.001). This indicates that early diagnosis of MT before invasion or metastasis is important for treatment of this malignancy.
FIGO, International Federation of Gynecology and Obstetrics; MT, malignant transformation.
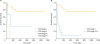
Fig. 3
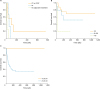
(A) Patients with stage II–IV who received adjuvant chemotherapy or CCRT had longer survival times than patients who received adjuvant RT alone or no adjuvant therapy (p<0.05). It implies that chemotherapy or CCRT may play a role in treating this malignancy. (B) Different survival in patients stratified by concentration of CA125 (cut-off values 43–116; 0: <43, 1: 43–116, 2: >116, p<0.005). (C) Different survival in patients grouped by tumor size ≥15.0 cm (0: <15.0 cm, 1: ≥15.0 cm, p<0.005).
CA125, cancer antigen 125; CCRT, concurrent chemoradiotherapy; RT, radiation therapy.
8. Tumor markers and tumor size
Serum cancer antigen 125 (CA125) levels were preoperatively measured in most patients (n=47); among them, 23 had CA125 levels greater than 35 U/mL (range, 0.8–1,699.7 U/mL). Serum SCC antigen levels were measured in 38 patients, and 24 patients had SCC antigen levels greater than 1.5 ng/mL. Serum carbohydrate antigen 19-9 (CA19-9) levels were measured in 12 patients and 5 patients had CA19-9 levels greater than 37.0 U/mL.
Carcinoembryonic antigen (CEA) levels were measured in 28 patients, and 11 patients had levels greater than 5.0 ng/mL. Hackethal et al. [15] reported no correlation between concentrations of tumor markers and FIGO stage; however, higher concentrations of squamous-cell-carcinoma antigen and CA125 (cut-off values, 43–116) were associated with adverse outcomes. In our study, tumor marker levels did not also correlate with the FIGO stage; however, higher CA125 levels (cut-off values, 43–116) were associated with adverse outcomes (Fig. 3B). A tumor size of ≥10 cm should be highly suspected for MT [16]. In our study, the mean tumor size was 10.8 cm, and a tumor size of ≥15.0 cm appeared to be associated with more aggressive disease (Fig. 3C).
DISCUSSION
Because of the rarity of MT to SCC and the complex components of MCTs, preoperatively distinguishing between these 2 conditions is extremely difficult. It generally occurs after the age of 40 years. In the present study, the median age at diagnosis of MT of MCT was 52 years, which tended to be higher than that of its benign counterpart [17181920]. Kashimura et al. [19] reported the patient age at differential diagnosis, with a mean age at diagnosis of 32.7 years for MCT vs. 50.8 years for SCC. The most common symptoms for this disease are abdominal pain, the presence of an abdominal mass [1920], and abdominal distension [20]. Occasionally, patients may present with torsion of the ovarian vascular pedicle or ovarian rupture requiring emergency surgery [8]. The duration of symptoms can vary; a symptom duration of 1–7 months before diagnosis was observed in our study. Hirakawa et al. [6] reported that 3 of 28 MCT patients had an antecedent history of abdominal tumors for 10–32 years, suggesting a long duration for MT in the pelvic cavity. Prolonged exposure to various carcinogens in the pelvic cavity might cause a malignant change in MCTs [17]. High-risk HPV infection may be associated with ovarian SCC [811]. Furthermore, we recently showed that high-risk HPV infection might be a causal factor for inducing MT of ovarian MCT to SCC [21]. We had also finished 4 patients with immunohistochemistry (IHC) & fluorescence in situ hybridization (FISH) from the uterine cervix to ovaries with 2 control groups for proving HPVs infection. We tested the tissue distribution of HPVs infection in the SCC-MCT samples, cervical cancer tissues, as well as their adjacent tissues from reproductive organs and associated pelvic/para-aortic lymph nodes. HPV capsid and HPV16/18 E6 proteins were highly detected in the tested samples (95%), which suggested broad HPV infection in the reproductive system of SCC-MCT and cervical cancer patients [21] (Fig. 4).
Fig. 4
HPV diagnosis by IHC analysis. HPV infection in cases 2 of SCC-MCT detected by IHC with antibodies for HPV capsid protein and HPV16/18 E6 protein.
HPV, human papillomavirus; IHC, immunohistochemistry; LN, lymph node; SCC-MCT, squamous cell carcinoma with mature cystic teratoma.

SCC antigen appears to be the most useful tumor marker for this disease. However, the usefulness of this antigen in the diagnosis of SCC remains controversial because positive rates of only 30%–67% have been reported [172223]. In our study, only 24 (46.1%) patients had increased serum SCC antigen levels. Therefore, serum SCC antigen alone is insufficient to exclude MT. By contrast, most reported cases of recurrence show increased SCC antigen levels, which usually precede the clinical disease by several months [2224]. Rim et al. [17] reported that a combination of patient age (≥40 years) and serum SCC antigen levels (≥2.5 ng/mL) was 77% sensitive and 96% specific for MT. In our study, elevated tumor serum marker levels (of SCC, CA125, CA19-9, and CEA) were observed in many patients, but they did not correlate with the FIGO stage. Due to our research aim was MT in mature dermoid cyst (no tumor markers sampling before operation in SCC and CA19-9) and retrospective survey (long time interval), there are many data were missing in SCC antigen and CA19-9. However, high CA125 levels, which were assessed according to the cut-off values (43–116 U/mL) reported by Hackethal et al. [15], were associated with adverse outcomes.
Imaging-related tumor characteristics that may assist in the detection of MT have been investigated. Kido et al. [14] reported that in malignant tumors arising from MCTs, a contrast-enhanced area of solid components and transmural extension and irregular invasion through the septa to the peritoneal area can be observed. In our study, preoperative imaging showed that 75% of patients had some solid portions in typical MCT lesions, and most of the malignancies were found around these solid portions.
Histologically, the tumor of the ovary was composed of a proliferation of polygonal cells arranged in a sheet pattern with keratinization. A few surface epithelial inclusion cysts, which were lined by a single layer of columnar epithelium with squamous metaplasia in part, were found in the ovarian cortex. Stepwise serial sections disclosed that the tumor nests were contiguous to the epithelium of inclusion cyst showing squamous metaplasia. The tumor was diagnosed as SCC arising from the epithelium of surface [25]. Park el al. [26] also reported in pure SCC ovary cancer notable for the absence of any associated dermoid cyst.
The prognosis for pure squamous ovarian carcinoma, independent of type, is poorer than that for ovarian epithelial cancers of all histologic types, according to most reports in the literature [27]. The overall survival of the patients with pure primary ovarian SCC reported by Pins et al. [28] was not significantly different from that of the 19 patients with malignant teratoma. All tumors of the patients with advanced ovarian SCC, who responded to chemotherapy and survived for over 2 years or longer were co-existed with dermoid cyst or endometriosis. There might be a difference in sensitivity to chemotherapy between pure-type ovarian SCC and ovarian SCC with dermoid cyst or endometriosis [29].
Although the size of MCTs can vary widely, MT correlates with increasing tumor dimensions. A tumor size of > or =10 cm should be highly suspected for MT [16]. In our study, the mean tumor size was 10.8 cm, and a tumor size of ≥15.0 cm appeared to be associated with more aggressive disease (Table 2).
Table 2
Demonstrating prognostic factors for SCC from MCT of the ovary in 7 previous series and 3 series of MT from ovarian dermoid cysts

| Author | No. of patients | Median/mean of age (range) | FIGO stage | Risk factors | Favorable factors |
|---|---|---|---|---|---|
| 1. Tseng et al. [22] | 26 | Median 51.6 (21–77) | I–IV | SCC >2 ng/mL | Early stage (I–II), optimal debulking |
| 2. Kikkawa et al. [20] | 37 | Median 55 (28–87) | I–III | Age ≥45, tumor size ≥99 mm, SCC/CEA measure under age/tumor size risk | Early stage (I–II), no residual tumor, grade 1, no VSI, α-mode tumor infiltration* |
| 3. Rim et al. [17] | 7 | Median 50 (19–71) | I–II | Postmenopause age, elevated SCC | Early stage (IA–IIB) |
| 4. Santos et al. [18] | 17 | Median 55 (37–75) | I–III | Old age, tumor size >10 cm | Early stage (IA–IIB) |
| 5. Hackethal et al. [15] | 126 | Mean 55 (19.0–87.0) | IA–IV | Age ≥50, tumor size ≥100 mm, stage, high SCC antigen, CA125 level | SCC <4.7 ng/mL, CA125 <43.0 U/mL, stage I favor prognosis, staging operation (lymphadenectomy in advanced disease improve the survival), omentectomy did not effect overall survival, chemotherapy with alkylating drugs, postoperative RT no benefit effect |
| 6. Park et al. [43] | 16 | Median 50 (29–75) | IA–IIIC | Age ≥50, tumor size >10 cm with some solid portion in MCT | Nil |
| 7. Gainford et al.† [45] | 33 | Mean 49 (19–87) | I–IV | Advanced stage | Stage I, platinum-based regimens, secondary debulking surgeries, second-line treatment with chemotherapy or RT alone seemed ineffective |
| 8. Sakuma et al.‡ [44] | 20 | Median 52.5 (29–77) | I–IV | Age >50 | Stage I–II, cytoreductive surgery (optimally), platinum/taxane chemotherapy, new regimens using nedaplatin |
| 9. Black et al. [32] | 9 | Mean 53.7 (22–74) | IA–IIIC | Age >50, tumor size ≥18 cm | Frozen section procedures, FOLFOX chemotherapy§ |
| 10. Our series | 52 | Median 52, mean 53 (29–89) | I–IV | CA125 level, tumor size ≥15 cm, solid components | Stage I, adjuvant treatment |
ANZGOG, Australia New Zealand Gynaecological Oncology Group; CA125, cancer antigen 125; CEA, carcinoembryonic antigen; FIGO, International Federation of Gynecology and Obstetrics; FOLFOX, leucovorin, fluorouracil, and oxaliplatin; GCIG, Gynecologic Cancer Intergroup; MCT, mature cystic teratoma; MT, malignant transformation; SCC, squamous cell carcinoma; RT, radiation therapy; VSI, vascular space involvement.
*α-mode of tumor infiltration: invasion of carcinoma cells into the stroma expansively with a well-defined border between tumor and stroma; †An ANZGOG and GCIG study in malignant transformation within ovarian dermoid cysts; ‡A retrospective study of 20 (15 with SCC) cases of malignant transformation arising from mature cystic teratoma of the ovary; §For mucinous adenocarcinoma.
In the case of grade, only grade 2 showed significant effect, but not grade 3. This might have been an artificial effect since there was a lot of missing information on patients' grade. We took the above significant factors and performed multivariate analysis. When grade, CA125 and stage (both as a binomial and a quadruple variable) were tested together, only stage was significant, and when stage was taken as a quadruple variable, only stages 3 and 4 were significant. Considering that grade may not be really a significant factor, we also performed multivariate analysis with only CA125 and stage. We found that the highest value of CA125 (>116 U/mL) was significant, so were stage as a binomial variable and stages 3 and 4 when quadruple.
Laparoscopic surgery is a recent novel technique for gynecologic surgery. An exploratory laparotomy is performed as indicated for suspected malignancy, because of the higher risk of tumor spillage of dermoid contents with laparoscopic procedures [30]. Successful laparoscopic removal of adherent MCTs without spilling their contents is frequently problematic, and a laparotomy should be performed to prevent inadvertent tumor upstaging by iatrogenic intraperitoneal rupture. Wen et al. [31] presented 2 cases of MT of MCT in which rapid postoperative progression occurred after intraoperative spillage of the tumor contents. Regardless of whether tumor dissemination correlates with intraoperative tumor rupture, Wen et al. [31] emphasized that in any patient with a preoperative diagnosis of MCT, the tumor should be removed completely intact to avoid possible iatrogenic complications and catastrophic events such as peritoneal dissemination of the tumor.
Although a frozen-section procedure is not the gold standard for MCT patients, it is a valuable tool and should be strongly considered if the patient or tumor exhibits any of the characteristics of malignant potential. In a series by Black et al. [32], malignant components within MCTs were diagnosed in frozen sections in 100% of cases. All of those patients subsequently underwent complete surgical staging. Thus, completion of the frozen-section procedure enabled the patients to avoid a second operation. Although up to 80% of malignancies arising from MCTs are SCC [15], Black et al. [32] suggested a higher incidence (approximately 50%) of MT to ovarian mucinous adenocarcinoma. This finding is clinically relevant because if ovarian mucinous adenocarcinoma is identified in frozen sections, an appendectomy would be completed as part of the surgical staging, whereas an appendectomy would not be necessary in other types of malignancy. Furthermore, Black et al. [32] closely studied MCTs that exhibited a carcinoid tumor as the malignant component. Although patients with carcinoid tumors do not need to be fully staged, some carcinoid tumors can exhibit an insular morphology, and these tumors have a higher likelihood of exhibiting malignant behavior and are associated with carcinoid syndrome [33]. Therefore, Black et al. [32] suggested that complete surgical staging, as well as optimal tumor debulking and adjuvant chemotherapy with folic acid, fluorouracil, and oxaliplatin (FOLFOX), could benefit patients with mucinous adenocarcinoma as the malignant component of an MCT. This is consistent with preclinical data on mucinous ovarian cancer cell lines and xenografts [3435]. In their series, FOLFOX was used only for mucinous histologies; therefore, the role of FOLFOX in treating other histologic subtypes of malignancy arising from an MCT remains unknown; thus, further research is warranted. FOLFOX-4 has shown activity in platinum/taxane-resistant heavily pretreated ovarian cancers across serous, mucinous, endometrioid, clear cell, and undifferentiated histologies [363738].
There is no consensus regarding adjuvant treatment and the effectiveness of chemotherapy or RT for MT of MCTs. We mainly used platinum-based chemotherapy in our study because of its activity against epithelial ovarian cancer and cervical SCC [394041]. Several previous studies have recommended combination chemotherapy with paclitaxel and carboplatin as active agents for MT of MCTs and have reported an extended progression-free interval in most patients [18424344]. An Australia New Zealand Gynaecological Oncology Group (ANZGOG) and Gynaecological Cancer Intergroup research observed 2 patients with a sustained remission after secondary debulking surgery. In light of this observation, this surgery should be considered in selected patients with relapsed disease. In contrast, second-line treatment with chemotherapy or RT alone seemed ineffective [45].
Our study had 18 stage IA SCC patients, all of whom received nondebulking or debulking surgery (n=9, each); 2 patients underwent surgery twice, with the second procedure being a debulking operation. Two of the 18 patients were lost to follow-up; one patient, who received debulking surgery without any adjuvant treatment, died; and 9 patients (5 for chemotherapy, 2 for CCRT, and 2 for RT) received adjuvant treatments. Tseng et al. [22] reviewed 26 cases of SCC and showed that the 2-year disease-free survival rate was 100%, 30%, and 0% for stage I or II, III, and IV patients, respectively. Dos Santos et al. [18] reported that the 5-year survival rate for adequately staged patients was 95%, 80%, and 0% for stages I, II, and III or IV, respectively. Therefore, a complete staging procedure and adjuvant therapy appears to be necessary even in patients with stage IA tumors. Tseng et al. [22] also reported that stage IIB–IIIC patients were treated with cisplatinum-based chemotherapy with or without sequential RT. Pelvic/para-aortic lymph node dissection is controversial because the tumor spreads by direct extension and/or peritoneal seeding, and metastatic lymph nodes are described in the literature. Dos Santos et al. [18] proposed whole-pelvis radiation and platinum-based chemotherapy for stage I–II patients because SCC is a radiosensitive tumor. Mandal and Badhe [46] reported MT of an MCT with metastatic deposits in the omentum. Removal of the entire tumor, in accordance with oncosurgical treatment principles, is essential, following which complete cytoreduction can further improve the outcome in these patients [46]. Other prognostic factors are tumor grade, growth pattern, capsular rupture, and vascular invasion [17]. Because of the rarity of this disease, there is insufficient data supporting the safety of fertility-sparing surgery, even in early-stage disease. Thus, complete surgical staging, as performed for ovarian cancer, is considered the safest procedure.
The FIGO staging applied to SCCs in MCTs does not clearly relate to the graduated outcome of the disease. A large ovarian mass suspected to be a mature teratoma should be more carefully managed in older patients. To the best of our knowledge, the present study is the largest clinical multicenter survey on this topic. This tumor was observed in postmenopausal and premenopausal women presenting with abdominal pain or a mass. The tumor size ranged from 10 to 400 mm in our study. Our data suggest that although MT is rare, it is more likely to occur in patients older than 52 years and in masses larger than 10.8 cm. Similar to most ovarian cancers, these tumors most frequently present at later stages and are thus difficult to treat. Therefore, the establishment of a revised classification of these tumor stages is highly recommended.
In conclusion, MT of MCTs to SCCs is rare and has a poor outcome. Early detection and complete surgical resection of the tumor, along with an early FIGO stage, are crucial to patient survival. Preoperative diagnosis of this malignancy is difficult. SCC arising in an MCT is an unusual disease for which there is little evidence to inform treatment; therefore, it remains a diagnostic dilemma for gynecological oncologists. The limited number of cases for analysis makes it difficult to establish definite conclusions regarding the appropriate adjuvant chemotherapy for this disease. However, combined platinum/taxane chemotherapy may lead to improved survival in advanced-stage disease. CCRT can be used to treat this malignancy in advanced stages. Our review of patients from multiple centers and the literature revealed that SCC usually occurs in postmenopausal women older than 50 years and is associated with large tumors (>10.8 cm) with solid components. In some cases, serum SCC antigen levels are increased, but these levels are an unreliable indicator of this malignancy. Intraoperative frozen sections should be examined in such cases to ensure that appropriate staging can be completed as necessary. Practically, we suggest collecting additional international data through cooperative research to create a new, more accurate staging system and to standardize treatment.
 XML Download
XML Download