

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Carcinosarcoma of the uterine corpus is a rare neoplasm, accounting for less than 5% of all uterine malignancies [12]. It is characterized by the presence of both epithelial and stromal malignant components. Immunohistochemical and molecular studies have suggested that the sarcomatous component is actually a metaplastic component derived from the carcinoma (combination tumor theory) [34]. Therefore, carcinosarcoma is believed to have biological behavior similar to high-grade endometrial carcinoma [4]. The clinical course of uterine carcinosarcoma is aggressive, contributing to 30% of uterine cancer mortality [1]. Although many clinicopathological factors, including the presence of a heterologous component, histologic types of the carcinomatous component, grade of the carcinomatous component, depth of myometrial invasion, and lymphatic and vascular space invasion, have been reported to be prognostic factors [56789], stage of disease has been the only definite independent prognostic indicator of survival in patients with uterine carcinosarcoma [789].
Necrosis is a significant prognostic factor of endometrial carcinoma [10], but its prognostic impact on carcinosarcoma is unclear. The magnetic resonance (MR) findings of carcinosarcoma include a heterogeneous appearance, including unenhanced areas, which possibly indicate necrosis [11]. The aims of this study are to confirm if the unenhanced regions on MR imaging (MRI) represent pathological necrosis and to explore the clinicobiological significance of these regions in patients with uterine carcinosarcoma.
MATERIALS AND METHODS
1. Patients
The records of 29 patients diagnosed with uterine carcinosarcoma treated at Kyoto University Hospital from 2003 to 2015 were retrospectively reviewed with the approval of the institutional ethics committee of Kyoto University Hospital. All patients provided informed consent. MR examinations with contrast enhancement were performed within one month before surgery for 22 cases. Only one patient did not undergo surgery because of her comorbidity.
2. Pathological review
All tumor samples were independently reviewed by at least 2 gynecologic pathologists, who were blinded to the patient data. The tumors were histologically classified according to World Health Organization (WHO) criteria. Clinical staging according to the International Federation of Gynecology and Obstetrics (FIGO) 2009 criteria was applied for all patients [12]. The suggestive staging according to imaging was performed for a patient who did not undergo surgery. Pathological necrosis was evaluated in 21 cases because the slides of a case were not available.
3. Evaluation of unenhanced areas on MRI
Two board-certified radiologists blinded to the clinical information retrospectively evaluated the size and unenhanced region of the tumors, using MR images obtained within 1 month before treatment initiation. The MR image sequences used for the evaluation were axial and sagittal T2-weighted images (T2WIs) and T1-weighted images (T1WIs) with and without contrast medium (Fig. 1A and 1B). Although a dynamic contrast enhancement study was performed, only the images obtained after 120 seconds of contrast material injection were used for evaluation.
Fig. 1
Contrast-enhanced MRI, macroscopic view, and histological specimen. (A) Sagittal image and (B) axial image showing a small unenhanced area ([A] pink line, [B] yellow line) in the tumor ([A] light blue line, [B] blue line). The average percentage of the tumor that is unenhanced is 9.6%. (C) Macroscopic view of the resected specimen demonstrating a large exophytic mass. Necrosis is seen in the center of the tumor. (D) Distinctive slice of the specimen, including a necrotic area. (E) Microscopic findings showing the presence of a necrotic area adjacent to a viable area and (F) viable tumor cells.
MRI, magnetic resonance imaging.

We evaluated the signal intensity of the tumor on T2WI compared to the uterine myometrium and assessed whether the tumor had a high signal intensity on T1WI, suggesting intratumoral hemorrhage using every slice of images. As for the evaluation of unenhanced region, the radiologists evaluated all the slices of tumors and selected the MRI sections in which the maximum diameters of the tumors were presented, by referring to subtraction images when possible. The unenhanced regions within the tumors were determined using a radiology workstation (Aquarius iNtuition Server; TeraRecon, Foster City, CA, USA) to identify the regions of interest by freehand depiction of the regions.
The subtraction images were made by subtracting the pre-enhanced images from the enhanced images on the workstation. When an unenhanced region was observed, the percentage of the unenhanced region within the selected slices was calculated on both axial and sagittal sections, and the average of both percentages was used for the analysis. Unenhanced regions on MR image were evaluated pathologically to determine if the areas represented necrosis in the corresponding specimen (Fig. 1C-1F).
4. Statistical analysis
Fisher's exact test was used to determine positive correlation of the unenhanced region on MRI to pathological necrosis and clinical factors (FIGO stage, grade of carcinomatous component, histology of sarcomatous component, tumor size, depth of myometrial invasion, lymphovascular space invasion (LVSI), ascites, and lymph node (LN) metastasis). The correlation coefficient was calculated using Spearman correlation analyses. Overall survival (OS) and progression-free survival (PFS) rates were calculated according to the Kaplan-Meier method, and differences were determined using the log-rank test. The prognostic significance of certain factors (FIGO stage, grade of carcinomatous component, histology of sarcomatous component, tumor size, depth of myometrial invasion, LVSI, ascites, LN metastasis, and unenhanced region on MR image) was assessed using the Cox proportional hazards regression model with SPSS version 22 software (SPSS Inc., Chicago, IL, USA). A p-value less than 0.05 was considered significant.
RESULTS
1. Clinical and histopathological characteristics of the cases
The clinical and histopathological characteristics are shown in Supplementary Table 1 and summarized in Supplementary Table 2. The patients' ages at presentation ranged from 46 to 82 years (median age, 65.3 years). Four patients were premenopausal. Three patients had been administered hormone therapy for breast cancer before the diagnosis of uterine carcinosarcoma. Before surgery, all patients had undergone hysteroscopy, which determined that the uterine cavity was filled with polypoid tumors in all cases. Of 29 cases of uterine carcinosarcoma, initial surgery was performed for 28 patients. The standard treatment comprised of primary total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic lymphadenectomy, and para-aortic lymphadenectomy with adjuvant chemotherapy (paclitaxel and carboplatin). Ten patients did not undergo pelvic and aortic LN dissection because of advanced age or the presence of distant metastasis, and instead underwent palliative surgery. The clinical FIGO stages were stage I in 16 (55%) patients, II in 2 (7%) patients, III in 7 (24%) patients, and IV in 4 (14%) patients. The greatest diameter of the tumors ranged from 1.5 to 18 cm (median, 7.6 cm).
Microscopically, the carcinomatous component was endometrioid adenocarcinoma in 12 (43%) cases, serous carcinoma in 5 (18%) cases, pure squamous cell carcinoma and poorly differentiated adenocarcinoma in 1 case each. Nine (32%) cases showed mixed type. Regarding the grade of the carcinomatous component, 7 (25%) cases were grade 1–2 adenocarcinoma and 21 (75%) cases were grade 3, which included serous and clear cell carcinoma. In the sarcomatous component, 17 (61%) cases were homologous, and 10 (36%) had heterologous elements. Myometrial invasion involving more than half of myometrium was identified in 13 (46%) cases, and LVSI was detected in 12 (43%) cases. Malignant cells in ascites were observed in 8 (29%) cases. LN metastasis was identified in 4 (14%) cases. During the follow-up period, 15 of 29 patients had recurrence, and 10 of the 24 cases died at 3.5 to 230.9 months (median, 53.3 months) after surgery.
2. Unenhanced regions on MRI reflect pathological necrosis
Regarding the signal intensity of T1WI and T2WI, the tumors were heterogeneous and had a higher signal intensity than the outer myometrium on T2WI and a lower-to-intermediate intensity on T1WI in most case. Contrast enhancement was observed in parts of the tumor for all cases. Five of 22 (22.7%) cases showed an extremely high signal intensity area in parts of the tumors on T1WI, which indicated intratumoral hemorrhage. Seventeen (77.3%) cases had unenhanced areas, which indicated suspected necrosis. Of 21 cases that were evaluated pathologically, unenhanced areas were present in 16 cases (76.2%). Pathological necrosis was identified in 14 out of the 16 cases. Four of the 5 cases that did not possess an unenhanced region on MRI showed absence of pathological necrosis. These findings indicated that unenhanced regions on MRI were significantly related to pathological necrosis (p=0.011; Fig. 1C-1F and Table 1). In 2 cases, which lacked pathological necrosis but had unenhanced regions on T1WI, the unenhanced regions reflected a cyst or hyalinization.

3. Unenhanced region on MRI predicts poor prognosis
Kaplan-Meier survival analyses were applied to evaluate the contribution of clinical factors, including pathological necrosis and the presence of an unenhanced region on MRI, to the OS rate. Although the presence of pathological necrosis was not significantly related to poor prognosis (p=0.704; Fig. 2A), the presence of unenhanced regions on MRI was significantly associated with poor prognosis when more than 10% of the tumor was unenhanced (p=0.019; Fig. 2B). For the PFS rate, pathological necrosis was not a significant prognostic indicator (p=0.672; Table 2). Unenhanced regions on MRI tended to indicate a poor prognosis when the percentage of the regions in the tumor was more than 10%, but this was not significant (p=0.143; Table 2). Stage was a significant prognostic indicator in both OS and PFS (p=0.022 and p=0.013, respectively; Fig. 2C and 2D). In the univariate analysis of other factors using the log-rank test, histopathologic high-grade of the carcinomatous component, tumor size more than 7 cm, presence of malignant cells in ascites, and presence of LN metastasis were significant poor prognostic factors in terms of PFS (p=0.003, p=0.046, p=0.029, and p<0.001, respectively; Table 2). In terms of OS, more than 10% of the tumor being unenhanced on MRI, as well as advanced stages, histopathologic grade 3 of the carcinomatous component, presence of malignant cells in ascites, and presence of LN metastasis correlated with a worse prognosis compared with less than 10% of the tumor being unenhanced on MRI, early stages, histopathologic grade 1 and 2 of the carcinomatous component, and absence of malignant cells in ascites, respectively (p=0.019, p=0.022, p=0.021, p=0.042, and p=0.002, respectively; Table 2).
Fig. 2
OS rate of uterine carcinosarcoma patients based on the presence of pathological necrosis (A) and more than 10% of the tumor being unenhanced on MRI (B). OS rate (C) and PFS rate (D) according to FIGO stage.
FIGO, International Federation of Gynecology and Obstetrics; MRI, magnetic resonance imaging; OS, overall survival; PFS, progression-free survival.
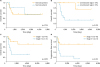
Table 2
Prognostic impact of clinical pathological factors using the log-rank test

To assess the clinical significance of unenhanced regions on MRI, the correlations of the ratio of the unenhanced region with tumor size and FIGO stage were evaluated. The percentage of unenhanced regions had a moderately positive correlation with tumor size (p=0.086, r=0.375; Fig. 3A) and a significantly positive correlation with clinical stage (p=0.028, r=0.469; Fig. 3B). Fisher's exact test revealed a significantly positive correlation of the unenhanced region on MRI to tumor size, but not to the other clinical factors (FIGO stage, grade of carcinomatous component, histology of sarcomatous component, depth of myometrial invasion, LVSI, ascites, and LN metastasis; p=0.007, p=0.367, p=0.101, p=1.000, p=0.085, p=0.387, p=1.000, and p=0.618, respectively; Supplementary Table 3). In Cox regression analyses, the univariate analysis of PFS showed that positive ascites cytology and the presence of LN metastasis were significant prognostic factors (p=0.035 and p=0.017, respectively; Supplementary Table 4). The multivariate analyses indicated that presence of LN metastasis was an independent prognostic factor associated with poor PFS (p=0.014; Supplementary Table 4). For OS, the presence of LN metastasis and more than 10% of the tumor being unenhanced on MR imaging were significant prognostic factors (p=0.022 and p=0.047, respectively; Table 3). The multivariate analyses indicated that both the presence of LN metastasis and more than 10% of the tumor being unenhanced on MRI were not independent prognostic factors associated with poor OS (p=0.096 and p=0.312, respectively; Table 3).
Fig. 3
Ratio of unenhanced regions on MRI is positively correlated with tumor size (A) and clinical stage (B).
MRI, magnetic resonance imaging.

Table 3
Univariate and multivariate analyses for OS rate using Cox regression model
DISCUSSION
Although carcinosarcoma of the uterus has a poor prognosis, the best treatment for this carcinosarcoma has not yet been determined [13]. A carcinosarcoma exhibits characteristic findings on MRI. Tanaka et al. [11] reported that carcinosarcoma typically appears as a large, exophytic, heterogeneous, high signal intensity mass on T2WI, and mostly contains strongly enhanced areas and unenhanced regions within the mass on T1WI, which could indicate necrosis. However, they did not confirm the unenhanced regions on MRI as representing pathological necrosis. Others have reported the same MRI findings of uterine carcinosarcoma [1415]. Our results are compatible with their findings. All cases showed an exophytic uterine endometrial mass with heterogeneous signal intensity. In our study, 17 (77.3%) cases had unenhanced areas, which almost coincided with pathological necrosis. That means that the presence of unenhanced areas within the mass, which implies the existence of necrosis, could be a frequent MR finding of uterine carcinosarcoma.
The definitive prognostic factors for carcinosarcoma of the uterus have been controversial. Galaal et al. [8] identified depth of myometrial invasion, stage, and pelvic node metastasis to be associated with poor survival. Stage appears to be an independent prognostic indicator of survival in patients with uterine carcinosarcoma [67]. It is uncertain whether age, endometrioid adenocarcinoma as a carcinomatous component, or absence of a heterologous component in the sarcomatous area are favorable prognostic factors [7]. Matsuo et al. [5] demonstrated that high-grade and a heterologous pattern are correlated with the worst PFS. In our study, log-rank tests indicated that FIGO stage, histological grade of the carcinomatous component, positive cytology of ascites, LN metastasis, and the presence of an unenhanced region on MRI were associated with poor OS. The univariate analyses using a Cox regression model identified LN metastasis and more than 10% of the tumor being unenhanced on MRI as poor prognostic indicators in OS. Although the multivariate analyses determined that neither of these factors was an independent prognostic factor, our findings suggest that semi-quantification of an unenhanced region on MRI, indicating tumor necrosis, is a prognostic indicator for uterine carcinosarcoma, in addition to stage, histological grade, LN status, and sarcomatous component.
Few reports have investigated the prognostic impact of the presence of necrosis. Rovirosa et al. [6] reported that the existence of pathological necrosis did not have a significant influence on OS. However, the methodology for evaluating necrosis is uncertain. For example, it has poor reproducibility, and excluding the presence of necrosis requires adequate sampling [10]. Therefore, we attempted to quantify the extent of necrosis in tumors using the unenhanced region on MRI, because an unenhanced region on MRI corresponded highly with pathological necrosis in our study. When the extent of tumor necrosis was semi-quantitatively assessed as either absent, focal (≤10% of the tumor area), moderate (10%–30%), or extensive (≥30%), the necrosis showed significant impact on prognosis of colorectal cancer patients in a volume-dependent manner [16]. Because of small numbers of patients in this study, we used 10% unenhanced region as the cut off value because this value categorized them clearly into favorable and poor prognosis groups. As a result, semi-quantification of the necrotic region (>10%) using MRI successfully predicted worse OS.
Unfortunately, it is very difficult to identify microscopically which component contributes to necrosis, because viable cells disappear in the necrotic region. However, by MRI findings, the sarcomatous component is suspected to be more likely to have hemorrhagic necrosis. Takemori et al. [14] reported that the sarcomatous component was more strongly enhanced than the carcinomatous component on contrast-enhanced T1WI, and this might be related to the prominent vascularity of the sarcomatous component. Ohguri et al. [17] also reported that the portions with high signal intensity in the early phase dynamic study corresponded histologically to sarcomatous components with prominent vascularity. Matsuo et al. [5] reported that not only did the carcinoma component play a leading role in tumor progression and survival, but also that the sarcoma component contributed markedly. They suggested that the effect of chemotherapy seems to vary according to the histologic combination of carcinoma and sarcoma components. These findings suggest that tumors with large unenhanced regions, which are related to poor prognosis, might predominantly comprise sarcoma. It is hypothesized that tumor necrosis is caused by chronic ischemic injury due to rapid tumor growth [18]. Tanaka et al. [11] also reported that only 2 of the 8 tumors that included an unenhanced area were smaller than 8 cm in maximum diameter. In our study, the presence of an unenhanced region correlated with tumor size and clinical stage. Therefore, necrosis seems to indicate uterine carcinosarcomas that have developed into larger masses. Necrosis is often accompanied by hypoxia, leading to the induction of hypoxia-inducible factors [19]. Ischemic regions contribute to tumor progression by inducing overexpression of hypoxia-inducible factors under hypoxic conditions [20]. These findings imply that unenhanced regions caused by necrosis likely represent a highly aggressive tumor with active proliferation.
There are several limitations of this study. First, our findings are based on a single-center study with a small sample size, which might have hindered identification of independent prognostic factors. Second, unenhanced regions on MRI can represent hyalinization or a cyst as well as necrosis. In fact, 2 cases had hyalinization and cyst formation in our study. Five of the 22 cases with a high signal intensity area in the tumors on T1WI had intratumoral hemorrhage. Although intermediate-to-high signal intensity on T1WI is helpful for diagnosing hemorrhagic necrosis [21], MRI is unable to strictly quantify necrosis.
In summary, unenhanced regions on MRI represent pathological necrosis and aggressive biology. Semi-quantification of necrosis using MRI is useful to predict the prognosis of uterine carcinosarcoma. Multi-center or larger studies are needed to validate the impact of the presence of an unenhanced region on MRI on prognosis of this rare, aggressive disease.
 XML Download
XML Download