

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) is the most lethal gynecological cancer [1]. EOC is predominantly a post-menopausal disease, most frequently diagnosed in women in their sixties [1]. Of the known risk factors for developing EOC, family history of ovarian cancer plays a dominant role. Notably, in a substantial proportion of families with clustering of EOC, germline mutations in either the BRCA1 or BRCA2 genes are encountered [2].
The spectrum of germline mutations in both genes amongst Jewish individuals, primarily but not exclusively of Ashkenazi origin, is limited: there are 2 BRCA1 mutations (185delAG and 5382InsC) and one in the BRCA2 mutation (6174delT) that are referred to as “founder Jewish BRCA mutations” [345]. The prevalence of these 3 predominant mutations has been reported in the general cancer-free Ashkenazi population (2.5%) [3], in unselected breast cancer cases (11%–12%) [6] and in unselected Israeli EOC cases (29%) [5]. 185delAG is also considered a founder mutation in Jewish individuals of Iraqi descent, in whom its prevalence in the general population is 0.5%.
The impact that BRCA gene mutations have on disease course, therapeutic response and overall survival (OS) in EOC is controversial. Most studies report an improved survival and better response to platinum based therapy among BRCA mutation carriers compared with non-carriers [478910111213], but others have shown that long-term survival is independent of BRCA status [14]. Notably, these data were published prior to the recent addition of poly (adenosine diphosphate [ADP]-ribose) polymerase (PARP) inhibitors to the arsenal of therapeutic tools in EOC patients who carry a germline or a somatic BRCA mutation [15].
Diagnosing EOC under 50 years of age is uncommon, and may increase the likelihood of identifying an inherited predisposition [2]. BRCA mutations are more prevalent in young EOC patients [916]. There is a paucity of data on the effect of young age at EOC diagnosis on disease course and outcome, as well as on the impact of BRCA mutations on prognosis in young EOC patients. The current study was undertaken to address these questions, taking advantage of the unique preponderance of BRCA mutations in the Jewish Israeli population.
MATERIALS AND METHODS
1. Patient population
Consecutive patients diagnosed with EOC, fallopian tube cancer, or primary peritoneal cancer at or under 50 years and treated at the Department of Gynecologic Oncology, Sheba Medical Center, Tel Hashomer, Israel between 1995 and 2011 were identified. Since 1996, all EOC patients at our institution are referred for genetic counseling and genotyping for the predominant Jewish BRCA mutations after completion of initial evaluation and treatment, usually during adjuvant chemotherapy. A large proportion are counseled and genotyped at the Oncogenetics Unit in the Sheba Medical Center.
2.Data collection
After obtaining institutional review board (IRB) ethical approval, medical records were reviewed and cross-referenced with databases at the Oncogenetics Unit to retrieve demographic and clinical data including patients' age at diagnosis, ethnicity, detailed family history of cancer, BRCA mutation status, medical and surgical history, disease stage and histology, CA125 levels at diagnosis and surgical outcome. Additionally, follow-up data on disease course including surgical outcome, chemotherapy, disease recurrence and re-treatment, follow-up and survival data were collected. Disease-free survival (DFS) was calculated from the completion of adjuvant chemotherapy to the date of first recurrence or last follow-up. OS was calculated from diagnosis to death, or last follow-up.
3. Statistical analysis
The prevalence of BRCA mutations in the study population, was extracted and compared with historical data available for the general Israeli EOC patient population [5]. A comparative analysis was performed between BRCA mutation carriers and non-carriers among study participants, across demographic, pathological, and clinical features. Survival data were compared using the Kaplan-Meier method and the log-rank test. The associations of clinical, genetic, pathological, and surgical variables with DFS and OS were assessed using the Cox proportional hazards method. Statistical analysis was performed on SPSS software (SPSS version 23; IBM Corp., Armonk, NY, USA).
4. Genetic testing
BRCA genotyping encompassed the 3 predominant Jewish Ashkenazi mutations in all cases, as previously described [17]. Since 2010 a NanoChip™ technology that genotypes for predominant and recurring BRCA mutations was applied [18]. All mutations were confirmed by sequencing. Genetic mutation testing is covered under the national health act and is performed free of charge for all women with the diagnosis of EOC.
Patients who tested negative for specific germline mutations were counseled about the possibility of harboring a private BRCA mutation and the availability of BRCA sequencing and extended genetic workup. Sequencing of BRCA was added to the public health coverage in 2012. Other extended testing, including multigene panel testing, is not covered and can be funded under private and supplementary health insurances.
RESULTS
Of 196 patients diagnosed with EOC at 50 years or younger and treated at the Sheba Medical Center during the study period, 186 records were found to have sufficiently complete data to be included in this analysis. Median length of follow-up (to last visit or date deceased) was 52 months (interquartile range, 31–92 months). Patients were 25–50 years old at diagnosis (mean, 44±5 years). Three patients (1.6%) were diagnosed under 30 years of age; 29 patients (15.6%) were 30–39 years old at diagnosis; and the majority (154, 83%) were in their forties.
The overwhelming majority of patients (162 patients—87.1% of the cohort) were Jewish, representing almost all patients in whom ethnicity was documented in the medical record. Only 2 Israeli Arabs were identified in this study population; for 22 patients no information on ethnicity was available on record. Of 104 patients for whom parental ethnicity was known, most were of Ashkenazi (n=48) or mixed Ashkenazi (n=10) descent—56% of the total. Thirty-eight patients (37%) were of non-Ashkenazi Jewish descent, including Balkan, North African and Asian (Iraqi, Iranian), or Yemenite descent.
Six patients had been diagnosed with breast cancer prior to EOC diagnosis. One hundred ten (59.1%) had family history of cancer in at least 1 or 2 first/second-degree relatives: breast cancer in 36 patients and ovarian cancer in 20 patients.
BRCA mutation status was unknown for 73 patients. Of 113 patients with known genetic testing results, 57 patients were BRCA mutation carriers (49.6%); this included 53 BRCA1 mutation carriers, 3 BRCA2 mutation carriers and 1 patient who carried mutations in both BRCA genes. Among BRCA1 mutation carriers, the most prevalent was the 185delAG mutation, identified in 32 patients (60%). There were also 6 5382insC mutation carriers and 4 Tyr978X mutation carriers. Eleven mutations identified were private BRCA1 mutations (a genetic mutation found only in a single family, as opposed to recurring or founder mutations which are found in unrelated families within a certain population and originate in a common ancestor). Six mutations were found in women under 39 years of age; 23 mutations in 40–44 years old patients and the rest were diagnosed in women 45–50 years of age. Binomial test showed a statistically significant difference when comparing the prevalence of BRCA mutations in the present study population, with data published for the general Israeli EOC population (29%, p<0.001).
BRCA mutation carriers had a higher prevalence of familial cancer history (84% vs. 61% in non-carriers, p=0.050). Specifically, a higher prevalence of breast and ovarian family cancer history was documented in BRCA mutation carriers compared with non-carriers (63% vs. 18%, p<0.010).
The majority of EOC in the study population were of serous histology (126, 68%); other cell types included endometrioid (24, 13%), mucinous (7, 4%), and clear cell (13, 7%) histologies. Of note, BRCA mutation carriers were more likely to have a serous tumor whereas non-serous histologies and specifically, clear cell tumors were more frequently represented among non-carriers (Table 1).
Table 1
Patient and disease characteristics in BRCA mutation carriers and non-carriers
Values are presented as number (%) or median (interquartile range). Most patients tested for 3 founder mutations: BRCA1-185delAG, BRCA1-5382insC, and BRCA2-6174delT.
*Other histologies included undifferentiated, anaplastic, mixed, and Brenner cell tumors; †p-value for serous vs. other (mucinous, endometrioid, and clear cell tumors); ‡p-value for early (stage I–II) vs. advanced (stage III–IV) disease; §p value for lnCA125 (plotted logarithmically due to extreme outliers); ‖Of 146 patients for whom residual tumor information was available.
NS, not significant.
In this young EOC population, 35% of patients were diagnosed at early stages (I–II) and 65% were diagnosed at advanced stages (III–IV). Although not statistically significant, stage distribution was skewed in favor of advanced disease in BRCA mutation carriers (64% vs. 52%, p=0.250); this was also reflected in higher CA125 levels at diagnosis when both groups are compared (Table 1 and Fig. 1).
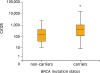
Fig. 1
CA125 levels in BRCA mutation carriers vs. non-carriers. CA125 levels in BRCA mutation carriers were significantly higher at diagnosis (median, 401 vs. 157; p=0.001) and had a wider interquartile range (122–1,100 vs. 39–415).
Over the course of their disease, patients received a mean of 3 lines of chemotherapy (0–12, standard deviation [SD]=2.7). Most patients recurred or had persistent disease (108 and 7 patients, respectively), but 71 patients (38%) remained disease-free over the entire follow-up period. Twenty-nine of these were BRCA mutation carriers, 27 were non-carriers, and the rest had unknown BRCA mutation status.
Five-year OS was 68% for BRCA mutation carriers and 65% for non-carriers (p=0.800). Univariate analyses showed early disease stage, maximal cytoreduction to no residual disease and non-serous histology were significantly associated with improved DFS and OS; however, BRCA mutations did not impact disease outcome (Fig. 2). Fifty patients with advanced (stage III–IV), high grade serous or endometrioid cancers with known BRCA mutation status were identified within the patient population. For this subgroup, as well, no significant association between BRCA mutations and either DFS or OS was found (Fig. 3).
Fig. 2
DFS (A) and OS (B) in BRCA mutation carriers vs. non-carriers. Median DFS was 46.2 months for non-carriers and 73.4 months for BRCA mutation carriers (p=0.910); median OS was not reached for non-carriers and was 213.7 months for BRCA mutation carriers (p=0.730).
DFS, disease-free survival; OS, overall survival.
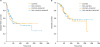
Fig. 3
DFS (A) and OS (B) in advanced, high-grade serous, and endometrioid ovarian cancer: BRCA mutation carriers vs. non-carriers. Disease outcome in a subpopulation of patients with advanced (stage III–IV), high-grade serous, or endometrioid ovarian tumors. Median DFS was 20.9 months for non-carriers and 21.2 months for BRCA mutation carriers (p=0.220); median OS was 63.5 months for non-carriers and 71.9 months for BRCA mutation carriers (p=0.720).
DFS, disease-free survival; OS, overall survival.

Multivariable analysis was confounded by an association of early disease stage and non-serous histology with lower residual disease at surgery (p<0.001, Chi-squared test). When residual disease at surgery was excluded from the analysis, multivariable Cox proportional hazards modeling demonstrated a significant association of both stage and histology with OS with a hazard ratio (HR) for death of 0.58 for non-serous histology (p=0.038) and 3.66 for advanced stage (p<0.001). However, in an analysis incorporating all variables, residual disease at surgery was independently associated with recurrence (HR=3; p=0.005) and non-significantly associated with survival (HR=2.3 for death, p=0.080) whereas other variables lost their association with outcome (Table 2). BRCA mutation status, which was not associated with residual disease at surgery (p=0.880), was not found to be independently associated with recurrence or survival in either analysis.
Table 2
HR for recurrence and death (Cox proportional hazards method)

DISCUSSION
This retrospective cohort study focuses on an under-researched patient population: young women with EOC. Patients were selected for diagnosis at age 50 and below, with a mean age of 44. The patient population described in the study is also unique in its ethnic composition. Being set in the major urban center of Israel, the vast majority of patients are Jewish, and specifically Jewish Ashkenazi.
Nearly half of the current study participants with known genetic testing results harbored a germline BRCA mutation. This is higher than the rate reported for consecutive ovarian cancer cases in most other studies, ranging from 10% to 20% across different populations [192021]. It is notably also higher than the 29% prevalence reported for an Israeli ovarian cancer patient population who were unselected for age or family history of cancer [5] or the 25%–40% reported for other Jewish ovarian cancer patient cohorts [162223]. These studies are summarized in a review analyzing BRCA mutations in Korean ovarian cancer patients [24]. The co-occurrence of 2 risk factors, young age and Jewish ethnicity, combine here to account for an exceptionally high rate of BRCA mutations. BRCA2 mutations were infrequent in this young ovarian cancer patient population, which is consistent with the older age at cancer diagnosis reported for BRCA2 mutation carriers in multiple studies [162526].
In the present study cohort, the majority (63%) of young EOC patients had a family history of cancer, and a substantial proportion had a family history of breast and/or ovarian cancer (34%), with notably higher rates of cancer history amongst families of BRCA mutation carriers (Table 1). It is well accepted that family history impacts on an individual's risk of cancer, a paradigm applicable to both individuals with and without identifiable mutations [2728]. The Hereditary Breast Cancer Clinical Study Group has previously shown a 1.2 (breast)–1.6 (ovary)-fold increase in cancer risk above baseline in BRCA mutation carriers for each first degree relative with cancer diagnosed under the age of 50 [29]. A family history of cancer also impacts on the age at diagnosis of BRCA-related cancers, with cancer diagnosed 8 years earlier in subsequent generations [30]. These observations are important in providing guidance for the timing of surveillance initiation and of risk reducing interventions in diagnosed BRCA mutation carriers as well as in high-risk women without an established genetic diagnosis. Of note, over one third of BRCA carriers in this study had no family history of breast or ovarian cancer, highlighting the need for genetic counseling and testing in all EOC in Israel, and specifically in those diagnosed by age 50 years, regardless of family history.
Over one third of the patients included in this study had no report of BRCA testing in their medical record despite a policy of 100% referral and full coverage of counseling and testing under the national health act. This, coupled with the high prevalence of BRCA mutations in the Israeli ovarian cancer population and particularly in the Jewish Ashkenazi population, highlights the importance of proactive counseling by providers on the importance of genetic testing. A low uptake of genetic testing for BRCA mutations has been reported by other groups [313233] and has improved over time with better acceptance [3435]. Uptake of genetic counseling and testing may be affected by various disease and patient characteristics [36373839]. Patients with rapidly progressive disease, for example, may have less opportunity to complete testing. Ethnic, cultural, and religious background may impact genetic counseling and testing acceptance; in Israel, orthodox patients are more likely to decline genetic testing as compared to secular ones, for BRCA as well as other diagnoses [40]. Low rates of uptake are often attributed to an overwhelming burden of information and competing tasks our patients and their supporters face [3132]. Working hand in hand with the oncogenetics services to provide patients with a counseling appointment as soon as ovarian cancer is diagnosed is imperative, in order to improve compliance and ensure that the majority of patients fall in with the international guideline for genetic testing. Making a genetic diagnosis in EOC cases is becoming increasingly important with PARP inhibitors taking the front stage in some treatment protocols and in many clinical trials.
BRCA mutation carriers showed a preponderance of high grade serous tumors; this histologic predilection is consistent with the literature [8]. Interestingly, histologic subtypes are distributed somewhat differently in the young EOC population studied herein than in the general ovarian cancer patient population [41], with a higher prevalence of non-serous histologies; this is particularly striking for non-mutation carriers, in whom clear cell histology—usually observed in under 3% of EOC—appears in 14% of cases (Table 1).
Outcomes for these young ovarian cancer patients were more favorable than reported for the general EOC population. Recurrence rate was only 57% for the study population over the course of follow-up, and median OS was 85 months. This may be partly explained by a more favorable stage distribution with 34% of patients diagnosed with stage I–II disease, as well as by a higher rate than usual of non-serous histologies (32%). Interestingly, BRCA mutation status did not have an independent impact on DFS or OS on either univariate or multivariate analysis (Fig. 2 and Table 2), contrary to previous reports suggesting BRCA mutation carriers may have better outcome compared to non-carriers [910111213]. The higher prevalence of early, non-serous tumors among non-BRCA carriers in this selected population may partly account for these results; in fact, Cox proportional hazards analysis pointed to histology and stage as stronger predictors of survival than BRCA status, as was residual macroscopic disease at surgery (Table 2). With this in mind, we looked at a subgroup of patients with advanced, high-grade serous, and endometrioid disease more representative of the typical ovarian cancer patient population; this was a small group consisting of only 50 patients, but again, no association between BRCA mutation and outcome was identified (Fig. 3). Our findings are in line with some reports on long-term survival in EOC patients, discounting an association with BRCA mutations [1442].
This study has several important limitations. As a retrospective cohort study, it has inherent flaws including access to important information that may be missing from medical records, loss to follow-up and widely varying follow-up periods impacting OS analysis. The study was conducted at a major tertiary gynecological cancer center, which has a broad referral base and is also public and accessible to all; however, it is ultimately a single institution study, with potential impact on patient selection, as evidenced by an overwhelming majority of Jewish patients. BRCA testing was missing in over one third of study patients, introducing a possible bias; both disease and patient characteristics may impact on the uptake of genetic testing. Some of the variables impacting on disease outcome, such as non-serous histology, early disease stage, and no macroscopic residual disease are interdependent, confounding the multivariable analysis. Mutation carriers tended to have more advanced disease at presentation, possibly skewing recurrence and survival results. Finally, the subgroup of patients with advanced, high-grade serous, and endometrioid tumors where BRCA mutation status would potentially have more impact was too small to allow multivariate analyses.
Despite these limitations, this report does shed light on an under-studied population of young EOC patients. Our findings show the frequency of BRCA mutations in young Israeli ovarian cancer patients to be about 50%, highlight differences in histologic subtypes and in disease patterns between BRCA mutation carriers and non-carriers, and support the hypothesis that BRCA gene mutation status may not independently impact disease course or survival in this young EOC population.
 XML Download
XML Download