

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the fourth most commonly diagnosed cancer in women worldwide, with developing countries facing the greatest burden of disease: 18/100,000 women per year contract the disease in developing countries, and a disproportionate amount of women die because of this disease [1]. Persistent genital infection with oncogenic human papillomavirus (HPV) appears to be the most important cause of cervical cancer [2345], but despite HPV's high prevalence (approximately 12.5% of women) [6], most women clear the virus before it can develop into cancer [7]. Thus, it is important to determine what factors play a role in the HPV infection or the cervical cancer following HPV infection.
Winkelstein first hypothesized in 1977 that smoking could be a risk factor for cervical cancer [8]. International epidemiological analyses have demonstrated that smoking is associated with an increased risk of squamous cell carcinoma [9]. However, the issue remains controversial today. In American cohorts where the female have a relative higher smoking prevalence ranging from 27.8%–32.4% [2101112], it has been reported that smoking is both protective against HPV infection [13], and conversely, that increased lifetime smoking duration is a risk factor for longer HPV persistence [12]. The female smoking prevalence in Asian studies also varies widely (38.4% in Japan [14], 19.8% in Thailand [15], 7.3% in South Korea [16], and 3.4% in China [17]). In these populations, the effect of smoking on HPV infection has also varied, with odds ratios (ORs) for smokers versus non-smokers ranging from 0.45 to 2.32 (Thailand and South Korea, respectively).
Moreover, the relationship between passive exposure to cigarette smoke and cervical neoplasia is less clear. Investigations conducted by Slattery and Trimble have demonstrated an increased cervical cancer risk among women exposed to passive smoke [1018]. However, an early study failed to show a consistent association between cervical intraepithelial neoplasia (CIN) and passive smoke exposure [11]. A few studies evaluating passive smoke exposure/active smoking and cervical neoplasia have not been consistent in their findings for limitations including small sample size of non-smoker controls and the status of active and passive history of smoking concurrently, lack of specific information on HPV and sexual behavior, etc.
Our study is a pooled analysis of 12 population-based, cross-sectional studies of cervical cancer across China. This is the largest analysis conducted to date in China, providing a unique opportunity to analyze the relationship between tobacco smoking, high-risk-HPV (hr-HPV) infection, and CIN grade 2+ (CIN2+) prevalence in this population.
MATERIALS AND METHODS
1. Participants
Cervical cancer screenings were conducted in 12 population-based, cross-sectional studies in 10 provinces in the People's Republic of China from 1999–2007 by the Cancer Institute of the Chinese Academy of Medical Sciences (CICAMS), Cleveland Clinic, International Agency for Research on Cancer (IARC), and Program of Appropriate Technology in Health (PATH). The 12 projects names were Shanxi Province Cervical Cancer Screening Study (SPOCCS)1–4, Screening Technologies to Advance Rapid Testing (START)2003–2007, and International Agency for Research on Cancer (IARC)-1–3, respectively. The individual project designs and their specific methods were outlined in detail elsewhere [1920212223242526], but to summarize, eligible women were sexually active, not pregnant, had an intact uterus, and had no history of CIN, cervical cancer, or pelvic irradiation. Written informed consent was obtained from all women. The human subjects review boards of CICAMS, Cleveland Clinic, PATH, or IARC approved these studies.
2. Procedures
Questionnaires that included information on socio-demographic characteristics, smoking history, reproductive history, menstrual factors, oral contraceptive use, and sexual behavior were administered by trained interviewers to study participants face-to-face. Questions on smoking habits included status of active (never, former, or current smoker [ever smoker]) and passive smoking (yes, no). Ever active smoker was defined as someone who reported any type of smoking for at least 6 months prior to the interview and included former and current smokers; passive smoker was defined as someone who lived in the same home as a smoking relative for 6 or more months. The gynecological examinations, specimen collection, cytology, and HPV DNA detection techniques have been described in the individual studies [2021]. All HPV tests were based on hr-HPV DNA detection by Hybrid Capture 2 (HC2) assay (Qiagen, Gaithersburg, MD, USA) [25].
3. Statistical analysis
Unconditional logistic regression was used to estimate the ORs and the corresponding 95% confidence intervals (CIs) of hr-HPV infection and CIN2+ based on smoking history. When calculating the ORs risk for CIN2+ and smoking status, the maximum likelihood estimates failed because the cell counts were small or zero in some studies; in these cases, exact logistic regression was used for analysis. Heterogeneity of the ORs among individual studies was tested using the χ2 based Cochran's Q statistic and the I2 statistic, and if the p-value was less than 0.05 and I2 less than 50%, there was no heterogeneity in the studies, or else a random effect model will be used for analysis.
The logistic models were constructed and adjusted by sexual and non-sexual confounding factors. Potential confounders included in these analyses were age (17–35, 36–49, ≥50), geographic area (rural, urban), education level (illiterate and primary school, middle school and above), age at menarche (≤15, ≥16), age at sexual debut (≤20, ≥21), lifetime number of sexual partners (1, ≥2), menopause (yes, no), parity (0, 1–2, ≥3), intrauterine device (IUD) (yes, no), oral contraceptives (yes, no), condoms (yes, no), sterilization (yes, no), husband had extramarital affair (yes, no) and passive smoking (yes, no). The models of CIN2+ prevalence were also adjusted for HPV infection status (+,−). Results were displayed in graphs with small diamonds and horizontal lines, representing the individual ORs and their corresponding 95% CIs respectively, while a bigger diamond was used to plot the overall OR for the pooled together. The individual women with the missing values were included by creating a category for “missing” for the relevant variable in order to avoid the exclusion of participants in the logistic regressions.
The interaction between active smoking or passive tobacco exposure was assessed for hr-HPV infection and CIN2+, the interactions were tested using likelihood ratio tests based on models with and without the interaction term(s). Linear trend chi-square tests were used to the homogeneity of the relationship between HPV infection and CIN2+ and the different smoking status (neither active nor passive smoking, only passive smoking, only active smoking, both active and passive smoking). Statistical analyses were performed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA) and Stata 12.0 (StataCorp. LLC, College Station, TX, USA).
RESULTS
Data from 12 population-based cervical cancer screening studies was pooled to analyze the relationship between smoking status, hr-HPV infection, and risk of CIN2+. A total of 17,582 women from 12 individual studies were included for this pooled study initially, and after excluding some due to inadequate HPV results, lack of smoking status or/and incomplete outcome data, and 16,422 women remained for the final analysis in relation to the hr-HPV infection and 15,791 in relation to the CIN2+.
Table 1 presents tobacco exposure and the prevalence of hr-HPV infection and CIN2+ in both the 12 individual studies and pooled overall. Women in the individual studies had a similar average age (ranging from 35.8 to 43.4 years old). The relatively low rates of ever smokers and higher rates of passive smokers were listed for each study. Five studies (SPOCCSIII-3, START2004, START2005, START2006, and IARC-1) reported an ever smoker rate of less than 1%, while most studies except IARC-2 (42.7%) reported a passive smoker rate of over 63.0%. The pooled rates of ever smokers and passive smokers were 1.9% and 73.7%, respectively. All studies except START2005 found a hr-HPV infection rate greater than 12%, resulting in a pooled HPV infection rate of 14.6%. CIN2+ prevalence in the individual studies ranged from 1.2% to 4.4%, with a pooled rate of 2.3%. Furthermore, the more specific number of active and passive smokers in the hr-HPV infection and and CIN2+ in each site were also shown in the the Supplementary Table 1.
Table 1
Tobacco exposure and prevalence of HPV and CIN2+ in 12 population-based cervical cancer screening studies
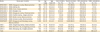
CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; IARC, International Agency for Research on Cancer; SD, standard deviation; SPOCCS, Shanxi Province Cervical Cancer Screening Study; START, Screening Technologies to Advance Rapid Testing.
*There were 15,791 women with complete pathology results.
![]()
Table 2 shows baseline characteristics for never smokers vs. ever smokers and passive vs. non-passive smokers in the pooled study. When compared to never smokers, ever smokers were more civic women. They were more likely to have a high educational level, to have had early sexual debut, to be post-menopausal and nulliparous, to have had multiple sexual partners and husbands with extramarital affairs, to use oral contraceptives, condoms or IUD rather than sterilization, to also be passive smokers, and to have hr-HPV or CIN2+. Compared to non-passive smokers, passive smokers were more likely to be between the ages of 36 and 49 years, to be from rural areas, to have a lower education level, to have had late age of menarche and early sexual debut, to be premenopausal, to have had multiple sexual partners and more than 3 parities, to use sterilization as a contraceptive, and to have HPV. Similarly, the associations between these baseline characteristics and the hr-HPV infection and CIN2+ were also evaluated, which additionally provided information on the potential confounding factors shown in the Supplementary Table 2.
Table 2
Baseline characteristics of women in pooled analysis, based on active or passive smoking status

Values are presented as number of subjects (%).
CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; IUD, intrauterine device.
*Smaller sample size than categorical groups due to missing values.
![]()
Fig. 1 displays adjusted ORs and 95% CIs for the relationship between active smoking and risk of HPV infection and CIN2+. There were no significant heterogeneity detected for the ORs between active smoking and HPV infection (I2=38%; p=0.100) or the CIN2+ (I2=12%; p=0.330) in each study. Active smokers had a statistically significant increased risk of HPV infection and CIN2+ than never smokers in pooled analyses. As showed in the part A and B of the Fig. 1, after being adjusted by multivariate, the relative likelihoods of both HPV infection and CIN2+ for ever smokers were statistically significant (OR=1.45; 95% CI=1.10–1.91, for HPV infection; OR=1.89; 95% CI=1.03–3.44, for CIN2+). However, a low active smoking rate and a limited number of CIN2+ cases in some individual studies led to wide and unstable 95% CIs of ORs.
 | Fig. 1Adjusted ORs and 95% CIs for the relationships between active smoking and risk of HPV infection (A) and CIN2+ (B) in the individual and pooled studies. (A) Logistic models were adjusted by age, area, education, age at menarche, age at sexual debut, sexual partners, menopause, parity, intrauterine device, oral contraceptives, condoms, sterilization, husband's affair, active, and passive smoking mutually; (B) Logistic-models were additionally adjusted for HPV infection.
CI, confidence interval; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; IARC, International Agency for Research on Cancer; OR, odds ratio; SPOCCS, Shanxi Province Cervical Cancer Screening Study; START, Screening Technologies to Advance Rapid Testing.
|
Fig. 2 shows the associations between passive smoking and risk of HPV and CIN2+ in individual and pooled studies. There were also no significant heterogeneity detected between passive smoking and HPV infection (I2=39%; p=0.080) or the CIN2+ (I2=0%; p=0.740). In the adjusted logistic models, passive and active tobacco exposures were adjusted mutually. Higher exposure to a smoking environment was slightly associated with a higher risk of HPV infection in the pooled study. Pooled OR and 95% CI for HPV infection was 1.11 (1.00–1.24) which was showed in the part A of the Fig. 2. No statistically significant association was found between passive smoking and risk of CIN2+ in the pooled analysis. The overall adjusted OR was 0.87 (0.68–1.12).
 | Fig. 2Adjusted ORs and 95% CIs for the relationships between passive smoking and risk of HPV infection (A) and CIN2+ (B) in the individual and pooled studies. (A) Logistic models were adjusted by age, area, education, age at menarche, age at sexual debut, sexual partners, menopause, parity, intrauterine device, oral contraceptives, condoms, sterilization, husband's affair, active, and passive smoking mutually; (B) Logistic-models were additionally adjusted for HPV infection.
CI, confidence interval; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; IARC, International Agency for Research on Cancer; OR, odds ratio; SPOCCS, Shanxi Province Cervical Cancer Screening Study; START, Screening Technologies to Advance Rapid Testing.
|
Table 3 presents multivariable ORs and 95% CIs for the associations between active smoking and risk of HPV infection and CIN2+ in the pooled analysis, stratified by passive smoking status. Passive smokers were more likely than non-passive smokers to be ever smokers, to have hr-HPV or CIN2+. Among passive smokers, the risk of hr-HPV infection (OR=1.39; 95% CI=1.03–1.89) and CIN2+ (OR=2.39; 95% CI=1.26–4.54) were significantly associated with active tobacco use, while no statistically significant association was observed among non-passive smokers. A significantly statistical interaction was found between active smoking and passive smoking in hr-HPV (p<0.001) and CIN2+ models (p<0.001). Joint ORs were also calculated by the adjusted regressions in order to evaluate the associations between 4 different combinations of active or passive smoking status with hr-HPV infection and CIN2+ in the Table 4. Compared with the neither active nor passive smokers, both active and passive smokers had a 1.57-fold (95% CI=1.14–2.15) increased risk of HPV infection and a 1.99-fold (95% CI=1.02–3.88) risk of CIN2+. There was a significant increased trend of the hr-HPV infection among the non-smokers, only passive smokers, only active smokers and both smokers (p<0.001), while there were still no significant trend between smoking and CIN2+ (p=0.086).
Table 3
Adjusted ORs and 95% CIs between active smoking and risk of hr-HPV infection and CIN2+ by passive smoking status in the pooled study

P for interaction between the passive and active smoking status: hr-HPV infection (p<0.001) and CIN2+ (p<0.001).
CI, confidence interval; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; hr-HPV, high-risk-human papillomavirus; OR, odds ratio.
*Logistic models were adjusted by age, area, education, age at menarche, age at sexual debut, sexual partners, menopause, parity, intrauterine device, oral contraceptives, condoms, sterilization, husband's affair, and active smoking, whereas CIN2+ models were additionally adjusted for HPV infection status.
![]()
Table 4
Adjusted ORs and 95% CIs between 4 different combinations of active or passive smoking status with hr-HPV infection and CIN2+ in the pooled study

Values are presented as adjusted OR (95% CI).
CI, confidence interval; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; hr-HPV, high-risk-human papillomavirus; OR, odds ratio.
*Logistic models were adjusted by age, area, education, age at menarche, age at sexual debut, sexual partners, menopause, parity, intrauterine device, oral contraceptives, condoms, sterilization, husband's affair, and joint smoking status, whereas CIN2+ models were additionally adjusted for HPV infection status.
![]()
DISCUSSION
This large multi-center cross-sectional study found a statistically significant association between active smoking and overall HPV or CIN2+ prevalence in the presence of passive smoking; a slightly significant association between passive smoking and overall HPV infection; and no association between passive smoking and CIN2+ regardless of active smoking status. Significant associations between active smoking and HPV infection and CIN2+ were observed among passive smokers. These results are based on the hypothesis that hr-HPV infection and CIN2+ have similar risk factors considering that hr-HPV infection is a necessary precursor of cervical cancer.
A controversial issue is becoming clear: smoking is certainly an independent risk factor of cervical cancer. A similar study conducted a pooled analysis of IARC multi-centric case-control studies and showed that ever-smokers had an excess risk of cervical cancer that persisted even after controlling for the strong effect of HPV and for other potential cofactors in the progression from infection to cancer [27]. Another large multinational and longitudinal cohort study prospectively assessed the role of tobacco smoking on the risk of developing intercultural communicative competence (ICC) and pre-cancer and confirmed the role of tobacco smoking as an important risk factor for both CIN3/carcinoma in situ (CIS) and ICC after taking into account HPV exposure (as determined by HPV serology). The low level of smoking in Chinese populations limited our ability to study the association between tobacco smoking and CIN3+/squamous cell carcinoma (SCC), but these and other studies have shown the magnitude of this association causes as much as a 2-fold increase in risk of either CINs or SCC/ICC [28293031]. The causes or mechanisms of this phenomenon are still unclear, but many studies have focused on tobacco-related carcinogens including nicotine, cotinine, benzo[a]pyrene, and 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone [32333435]. Given the importance of HPV infection in the progression of the cervical cancer, our study explored the role of tobacco on the risk of contracting HPV, and it showed that active smoking produced a 1.45-fold increased risk of contracting HPV, but after adjusting for HPV status and sexual behavior risk factors, the risk of CIN2+ increased to 1.89-fold, indicating that tobacco is related to CIN2+ partly because it increases the rate of HPV infection. There may be residual confounding that is responsible for these findings; for example, another study suggested that smoking could appear to increase the risk of acquiring a cervical HPV infection, because of the confounding effect of risky sexual behavior, which is strongly correlated with smoking [36].
The risks of HPV infection and CIN2+ for passive smokers were estimated by the similar confounding including the active smoking, but the risks were different with those for active smokers. Passive smoking mildly increased the risk of HPV infection but not the risk of CIN2+ following infection; this may be because passive smokers who test HPV positive at one time are more likely to clear their infections, whereas CIN2+ cases develop from persistent infection. However, the interaction between passive and active smoking was statistically significant; that is, active smokers who are also passive smokers have an even higher risk of HPV or CIN2+ than active smokers who are not exposed to secondhand smoke. However, few studies reported the active smoking, passive smoking and HPV infection. Consistent with our study, the pooled data from the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort showed active smoking was a definite risk factor on cervical lesions, but passive smoking could not be detected as an independent risk factor in the absence of active smoking [2837]. Another community-based case-control study found second-smokers had no significant risk compared with non-smokers, but second-smokers with a lifetime exposure of more than 20 pack-year cigarettes had a 7-fold increased risk (adjusted OR [95% CI]=7.2 [2.5–20.6]) [38]. Additionally, a study with high-grade squamous intraepithelial lesion (HSIL)/low-grade squamous intraepithelial lesions (LSIL) as the main outcome found the African-American women with a passive smoke exposure for more than 1 year had a elevated risk compared with the never exposure (adjusted OR [95% CI]=1.5 [1.0–2.2]), but the White women did not have the same results (adjusted OR [95% CI]=1.4 [0.7–2.8]) [39]. Due to the limited number of cancer cases, further large epidemiological studies, including more cervical cancer and pre-cancer cases, are needed to confirm these results.
The major strengths of our study were its large size and the use of similar questionnaires across individual studies such that important risk factors could all be adjusted in the same way. However, our study also has some limitations. First, smoking behavior was based on self-report in questionnaires rather than by detection of cotinine level, but agreement between self-report and urine cotinine level tended to be high (kappa=0.872) [40]. Secondly, we did not collect information about second-hand smoke from the workplace or other locations, only smoke from family members living together. Thus, neither the duration nor the intensity of passive smoking could be estimated, and the dose-dependent relationship could not be obtained. Thirdly, active smokers were not divided between those who purchased commercial cigarettes and those who smoked home-grown tobacco leaf (although the proportion of the home-grown tobacco smokers was low), but as the various additives in commercial cigarettes may cause additional harm to the health, this study may have underestimated the risk of the tobacco. Fourthly, HPV result in the pooled analysis was based on the detection by HC2 test, which cannot discriminate individual genotype, the effects of the smoking on the risk of the specific hr-HPV infection cannot be evaluated in our study. Finally, our study was based on a relatively small number of ever smokers, especially in each individual study, so our results may have been skewed by a few smokers.
Overall, this large, cross-sectional study shows a significant association between the risks of HPV infection and CIN2+ and active smoking. However, our results suggest a hazardous effect of active smoking against risk of cervical cancer who is both active and passive smokers. However, given the low rate of active smoking, principally by prevalence of the CIN3+ or SCC, larger sample size studies with more active smokers and HPV/CIN2+ cases are needed to elucidate the roles of active and passive tobacco smoking in the etiology of cervical cancer.
Since smoking is a modifiable health behavior, considerable public health benefit can be derived from availing ourselves of early opportunities for prevention and control, so the anti-smoking campaign and regulations launched by relative department in local area currently is really a good beginning.
 XML Download
XML Download