

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Radical hysterectomy with pelvic node dissection (RHND) is widely accepted as a safe and mainstay surgical treatment for cervical cancer, especially in the early stages. However, in the absence of postoperative adjuvant therapy, a significant proportion of patients will develop relapse and die from this cancer, even in selected early stage patients [12]. It is now well established from several prior studies that clinicopathologic factors (such as pelvic node metastasis, large tumor size, and deep stromal invasion [DSI]) influence the oncological outcomes after RHND for early stage cervical cancer [1234]. In addition, data from several large retrospective studies and 2 randomized clinical trials by the Gynecologic Oncology Group (GOG) (92 and 109), on adjuvant therapy (radiation or concurrent chemoradiation) have demonstrated improvement in oncological outcomes, a principle which now guides the current standard of surgical care for early stage cervical cancer [12567].
Most oncologists try to give adjuvant therapy as soon as clinically possible after the removal of the primary cancerous tumor. However, patients occasionally face a delay in starting their adjuvant therapy due to many factors including comorbid medical diseases, surgical complications, and availability of radiation facilities [891011]. In less developed countries such as Thailand with a rather high incidence of cervical cancer and limited resources in many settings (such as a shortage of radiation oncologists and/or equipment), a delay in starting adjuvant therapy is a major public health problem.
Various studies have proposed that the time interval (TI) from surgery to adjuvant therapy (radiation, concurrent chemoradiation, or chemotherapy) can have an impact in many types of cancer such as breast, colorectal, endometrial, head and neck cancers, and glioblastoma [89101112]. Ahmad et al. [12] studied 195 endometrial cancer patients who received postoperative whole pelvic radiation and found that a delay in radiation therapy (RT) of >6 weeks was an independent significant predictor for poor disease-specific survival (p<0.005) and a marginally significant variable for decreased local control. However, several other studies have found that delaying adjuvant therapy did not affect the clinical outcomes in cancer patients after surgical treatment such as soft tissue sarcoma, breast, and gastric cancers [131415].
To date, there have been no reliable scientific studies examining whether delaying adjuvant therapy after RHND is associated with poor oncological outcomes of early stage cervical cancer. Neither has the optimal time from RHND to initiating adjuvant therapy been examined. Thus, to address these research gaps, we performed a retrospective analysis to evaluate the effect of timing of adjuvant therapy on oncological outcomes in patients with early stage cervical cancer treated with RHND.
MATERIALS AND METHODS
After the Institutional Ethic Committee of the Faculty of Medicine, Prince of Songkla University approval, we identified 125 patients with International Federation of Gynecology and Obstetrics (FIGO) stage IA2 or IB1 cervical cancer who received adjuvant therapy (radiation or concurrent chemoradiation) after RHND at Songklanagarind Hospital between 1987 and 2016. Then, through a review of both inpatient and outpatient medical records, patients with squamous cell carcinoma, adenocarcinoma (AC), and adenosquamous carcinoma histology were identified. Patients diagnosed with other histological cell types (n=6), who were lost to follow-up (n=5), who received chemotherapy only (n=2), or whose date of adjuvant therapy initiation was missing (n=2) were excluded. The remaining 110 patients constituted the study group.
Details on clinicopathologic variables and clinical data from the medical records (age, tumor size, stage, histology, lymph-vascular space invasion [LVSI], DSI, lymph node status, parametrial involvement (PI), vaginal involvement, type of adjuvant therapy, treatment period, and oncological outcomes) were considered for the data analysis.
Clinical stages and histological tumor types were classified according to the revised FIGO 2009 and World Health Organization criteria. During the study period, whole pelvic radiation was used as an adjuvant therapy after RHND following certain indications (when a patient's pathological report displayed any of the following prognostic factors: PI, pelvic node metastasis, or positive surgical margin). However, following the year 2000, postoperative treatment protocols were based on pathological findings classified into 3 groups: low-, intermediate-, and high-risk groups, these being based on eligibility for GOG 92 and GOG 109 [17]. Patients with PI, pelvic node metastasis, or positive surgical margin were classified in the high-risk group. Patients with 2 or all of tumor size ≥4 cm, LVSI, or DSI were classified into the intermediate-risk group. Patients within the high-risk group were recommended to receive postoperative adjuvant concurrent chemoradiation therapy (CCRT), received the following treatment: 45–50 Gy of external beam RT in 1.8 or 2.0 Gy fractions once daily for 5 days per week with 40 mg/m2 cisplatin weekly±intracavitary radiotherapy (ICRT) or intracavitary brachytherapy. However, in the high-risk group, patients who either had poor performance status or refused additional chemotherapy received pelvic RT alone. Patients within the intermediate-risk group were recommended to undergo adjuvant 45–50 Gy of RT alone. Patients without any risk factors were considered to be in the low-risk group, and did not receive adjuvant treatment. All patients received definitive external beam RT with either a Cobalt-60 or a megavoltage linear accelerator. The parallel opposing field or 4-field box technique was used. The treatment volume encompassed tumor bed, internal iliac lymph node, external iliac lymph node, and common iliac lymph node when the pelvic lymph node was positive. Whenever the common iliac lymph node was involved, the treatment volume covered the para-aortic lymph node. If brachytherapy was performed, the brachytherapy dose was prescribed at 0.5 cm from the vaginal surface, and the proximal 4–5 cm of vagina was treated. For the high dose rate, the 3 fractions of ICRT were followed by a weekly fraction of 5–7 Gy. If the patients was treated at the low dose rate, the accumulative dose at 0.5 cm from the vaginal surface was limited to approximately 70 Gy. After complete treatment, all patients received follow-up every 3 months in the first year, every 4 months in the second year, every 6 months in the third to fifth years, and then yearly thereafter [1617].
The TI from RHND to starting adjuvant therapy (radiation or concurrent chemoradiation) was calculated as the time (in weeks) from the day of the RHND to the day when the patient received the first dose of RT. The primary outcome of the study was the impact of TI on recurrence-free survival (RFS) and overall survival (OS). RFS was defined as the time between the date of the operation and the date of recurrence, and OS from the date of the operation to the date of death or last contact. Patients who were lost to follow-up or did not experience an event during follow-up were considered to be censored at the latest date at which their status was known [17]. TI was analyzed as binary variables by grouping into ≤4 vs. >4 weeks. We also analyzed the impact of a cut-off TI 6 weeks based on the GOG 92 study [1]. Differences in clinicopathologic data across the different timings of adjuvant therapy were evaluated using the χ2 test. Univariate analyses of RFS and OS were performed using the Kaplan-Meier method. A multivariate Cox model for RFS was constructed by initially including TI (≤4 vs. >4 weeks) together with histology and an interaction term between histology and time, since it was thought possible that the effect of TI might be different in the 2 histological main types (squamous cell carcinoma and AC/adenosquamous cell carcinoma [ASC]). Other variables that were potential factors for RFS, namely tumor size, LVSI, DSI, lymph node status, PI, and vaginal involvement were then included and the model refined using backward removal guided by change in log likelihood of successive models. DSI, PI, and the interaction between histology and time remained significant, but with a significant time effect only in squamous cell carcinoma histological type. P-values below 0.05 were considered statistically significant. All analysis was done using STATA version 14 statistical software (StataCorp., College Station, TX, USA).
RESULTS
We identified 110 patients with early stage cervical cancer (3 stage IA2 and 107 stage IB1) who received adjuvant therapy (RT=83, CCRT=27) after RHND. The mean age at diagnosis for all patients was 49.0 years (range 24.0–74.0). Most (67.3%) had squamous cell carcinoma. The median TI was 4.5 weeks (interquartile range [IQR]=2.9–5.6 weeks), with 50 (45.5%) and 91 (82.7%) patients receiving adjuvant therapy within 4 and 6 weeks, respectively. The baseline clinicopathologic characteristics of the 110 patients according to TI (≤4 vs. >4 weeks) from surgery and adjuvant therapy are shown in Table 1. The 2 TI groups did not differ in age, tumor size, stage, histology, LVSI, DSI, lymph node status, vaginal involvement, or adjuvant therapy. However, patients who received adjuvant therapy within 4 weeks after their RHND were more likely to have PI (p=0.020). Patients who received adjuvant therapy within 4 weeks after RHND were more likely to have received treatment before the year 2004 (p<0.001). Furthermore, when we used the new cut-off TI of 6 weeks, the 2 TI groups (≤6 vs. >6 weeks) did not differ in any clinicopathologic characteristics (data not shown).
Table 1
Patient characteristics according to TI (≤4 weeks vs. >4 weeks) from surgery to adjuvant therapy

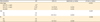
The median follow-up time of our study was 69.6 months (IQR=37.9–111.8 months). At the time of analysis, 20 (18.2%) of the 110 patients had had disease recurrence. Characteristics of 20 patients with recurrence according to TI (≤4 vs. >4 weeks) from surgery to adjuvant therapy are showed in Table 2. There were no significant differences in between the 2 groups. The median time from the RHND to recurrence was 38.1 months (IQR=25.5–77.8 months). The 5-year RFS of the whole population was 85.6% (95% confidence interval [CI]=76.4–91.4). The 5-year RFSs were 89.2% (75.9–95.4) and 83.2% (72.7–89.9) for patients whose TI was equal to or less than 4 and 6 weeks, respectively, and 81.0% (65.0–90.2) and 100% for patients whose waiting time was more than 4 weeks and 6 weeks, respectively (p=0.723 and 0.241, respectively). On univariate analysis, only histology (p<0.001), DSI (p=0.029), and PI (p=0.014) were significantly associated with 5-year RFS (Table 3). Table 4 shows the results of multivariate analysis of TI (4 weeks) from surgery to adjuvant therapy in relation to histology regarding RFS. DSI (p=0.037), and PI (p=0.002) were identified as independent prognostic factors for RFS, together with the interaction between TI and squamous cell carcinoma histology (p<0.001). In patients with squamous cell carcinoma, a TI longer than 4 weeks was significantly associated with a worse RFS (hazard ratio [HR]=15.8; 95% CI=1.4–173.9; p=0.024). Because there were very few patients with recurrence among patients with a TI longer than 6 weeks, the impact of this cut-off point could not be evaluated.
Table 2
Recurrent patient characteristics according to TI (≤4 weeks vs. >4 weeks) from surgery to adjuvant therapy
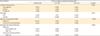
Table 3
Univariate analysis of 5-year RFS and 5-year OS

Table 4
Multivariate analysis of TI from surgery to adjuvant therapy in relation to histology regarding RFS
AC, adenocarcinoma; ASC, adenosquamous cell carcinoma; CI, confidence interval; DSI, deep stromal invasion; HR, hazard ratio; LR, likelihood ratio; PI, parametrial involvement; RFS, recurrence-free survival; SCC, squamous cell carcinoma; TI, time interval.
*,†Values within variables not having a superscript in common differ significantly (p-value <0.05, Wald test).
The 5-year OS of the whole population was 94.1% (95% CI=86.3–97.5). When the population was subdivided into TI groups of equal to or less, or longer than 4 and 6 weeks, the 5-year OSs were 90.9% (77.5–96.5) and 93.2% (84.3–97.1) for patients whose TIs were equal to or fewer than 4 and 6 weeks, respectively, and 97.2% (81.9–99.6) and 100% for patients whose TIs were more than 4 weeks and 6 weeks, respectively (p=0.486 and 0.327, respectively). On univariate analysis, only tumor size (p=0.023), and PI (p=0.003) were significantly associated with 5-year OS (Table 3). Again, because there were very few deaths in our study, multivariate analysis of clinicopathological prognostic factors and OS according to cut-off point of TI from surgery and adjuvant therapy (4 and 6 weeks) could not be performed.
DISCUSSION
Adjuvant therapy (radiation or concurrent chemoradiation) after RHND has been well established as the standard of care for intermediate- and high-risk early stage cervical cancer for almost 20 years [17]. Recommendations from clinical trials (including the GOG 92 study) for timely adjuvant therapy (within 4 to 6 weeks postoperatively) have been suggested, however no published scientific or clinical data support an exact time frame yet [17]. The conceptual role of adjuvant therapy after complete surgical resection is to control residual subclinical disease [3918]. The TI from surgery to adjuvant therapy may provide an opportunity for micrometastases to proliferate. Data from several animal model studies suggest that surgery may lead to early accelerated growth of micrometastases and the stimulation of angiogenesis by the release of circulating growth factors or reduction in angiogenesis inhibitors (such as angiostatin) [91920]. Furthermore, the stress response after surgery might induce a favorable environment for cancer progression in the early postoperative phase [1821]. So, it seems logical that early initiation of adjuvant therapy might increase the chances of eliminating any residual tumor cells before they have an opportunity to begin metastasizing, and, thereby, obtain improved oncological outcomes.
In our present analysis, the median TI from RHND to adjuvant therapy of 110 early stage cervical cancer patients was 4.5 weeks, and the majority of patients (82.7%) received adjuvant therapy within 6 weeks, as recommended by the GOG 92 study [1]. The impact of the TI from surgery to adjuvant therapy (radiation or concurrent chemoradiation) has been studied mainly in breast, endometrial, and head and neck cancers [101112132223]. Several retrospective cohort studies have found that a longer TI is associated with poor oncological outcomes of these cancers [10111222]. Recently, a study in 308 endometrial cancer patients found that delay (≥9 weeks) in beginning adjuvant RT after hysterectomy was associated with poor survival outcomes [23]. However, the association between the timing of adjuvant therapy after RHND in cervical cancer and oncological outcomes had not previously been reported. We found that delay in the beginning adjuvant therapy after RHND beyond 4 weeks might result in poorer RFS in patients with squamous cell carcinoma while patients with AC or ASC did not show any detriment from delay in administering adjuvant therapy. This result may be explained by the fact that the effect of TI of 4 weeks on oncological outcomes is more efficient in patients with squamous cell carcinoma, who have a better prognosis than those with AC or ASC [1624]. In addition, we could not detect any effect of TI (4 or 6 weeks) from RHND to adjuvant therapy on OS in patients with any histological cell types. These results may be related with the small sample size in our study. Another possible explanation for these results may be that all patients in our study had early stage disease with good prognosis and favorable outcomes after RHND with 5-year OS of 94.1%. So, in our study, the number of patients might have been inadequate to determine an effect of TI on OS.
This is the first scientific report to demonstrate the impact of timing of adjuvant therapy in cervical cancer on RFS. However, the impact of TI from surgery to the beginning of adjuvant therapy on oncological outcomes were not demonstrated by previous studies [1315]. A study by Cèfaro et al. [13] examined the effect of delaying RT after conservative surgery on the risk of local recurrence in 969 women with early stage breast cancer, and found that the TI from surgery to RT was not associated with local recurrence. The reason for the discrepancy is not clear. Thus, further work with larger number of patients with early stage cervical cancer including long term follow-up and/or using different cut-off points for the initiation of adjuvant therapy is needed before any definite conclusions.
To date, no previous study has investigated factors related to the delay of adjuvant treatment after RHND for cervical cancer. Our study found that PI and treatment period were all identified as factors that had an impact on the timing (≤4 vs. >4 weeks) of adjuvant therapy. These relationships may partly be explained by the decision of the involved radiation oncologist to initiate RT earlier in patients who are at especially high risk or fragile, as also noted in a previous study [8]. Bos et al. [25] reported that factors associated with starting treatment after 8 weeks in 6,620 patients with stage III colon cancer were older age, emergency resection, anastomotic leakage, referral to another hospital for adjuvant chemotherapy, and prolonged postoperative stay. Recently, another study found that laparoscopic surgery increased the chance of early adjuvant therapy in colonic cancer [18].
Several methodologic limitations merit comment. First, the study was a retrospective analysis with a relatively small number of patients, and thus potential confounding biases and important data (such as postoperative complication, surgical procedure, social factors, and medical comorbidities) might have been missed in the analysis. Second, this study was limited by its using historical data, single center, which may not accurately reflect the condition of the general population. So the results should be interpreted with caution.
In conclusion, despite its limitation, this study provides vital information that for early stage squamous cell cervical cancer, delay in administering adjuvant therapy after RHND beyond 4 weeks is associated with inferior RFS. Further larger-scale cohort studies are needed to confirm our results. Oncologists may need to consider timing more carefully when discussing adjuvant therapy after RHND with early stage cervical cancer patients especially those with squamous cell carcinoma.
 XML Download
XML Download