

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stage IB–IIA cervical carcinoma can be equally cured either by radical surgery or radiotherapy (RT). Albeit such treatment policies show the same efficacy, they carry a different morbidity, especially when surgery is followed by adjuvant pelvic irradiation. Our randomized trial performed between 1986 and 1991 in 343 patients confirmed such statements [1]. Nonetheless there is still an ongoing debate regarding the optimal treatment for these patients, since in the last decade at least 4 non-randomized studies were published, of which 3 seem to observe a significant survival advantage for surgical treatment compared to RT (Table 1) [2345].
Table 1
Recent literature comparing surgery vs. RT in stage IB–IIA cervical cancer

Therefore, data of our randomized trial were updated to December 2013 and reanalyzed in order to assess long-term survival and morbidity and pattern of relapse between the 2 treatment modalities.
MATERIALS AND METHODS
In the trial's protocol, patients with stage IB–IIA cervical cancer were randomized to radical surgery (Piver-Rutledge class III or Querleu-Morrow class C2 radical hysterectomy plus pelvic lymphadenectomy extended to level 2) or external RT (18 MV photon beam) with 4 portals plus brachy RT (1 caesium-137 LDR insertion) with a median total dose at point A of 76 Gy (range 70–90Gy). Details of patient selection and randomization, of surgical and radiotherapeutic techniques are available in our previous publication [1].
Patients who had at least 1 of the following pathological risk factors received adjuvant RT: surgical stage greater than pT2a, less than 3 mm of uninvolved cervical stroma, tumor cut-through and lymph node metastases. Adjuvant RT consisted of external pelvic irradiation (18 MV X-rays) with the multiportal technique, 1 fraction of 1.8–2.0 Gy daily, with a total dose of 50.4 Gy over 5–6 weeks. The paraaortic region was irradiated in case of common iliac or paraaortic nodes metastases with a dose of 45 Gy over 5 weeks. Complications were classified according to the Chassagne glossary [6]. The primary outcomes were 5-year overall survival (OS) and complications rate. The secondary outcome was disease recurrence.
1. Statistical analysis
The minimum detectable difference in survival and morbidity was defined as 15% for α=0.05 and 1-β=0.80. Chi-square test with Yates' continuity correction was used to test the association between discrete variables. Quantitative data were compared by 1-way analysis of variance.
Survival curves were calculated by the life-table method and compared by the log-rank test. A significance level of 95% was chosen. Survival and relapses were analyzed by intention to treat.
We analyzed the rate of complications by the actual treatment delivered to each patient so that the type and cause of morbidity associated with each treatment could be accurately assessed. Multivariate Cox regression analysis was employed to assess the effect of cervical size, age, International Federation of Gynecology and Obstetrics (FIGO) stage, histological type, grade of differentiation, radiological lymph-node status, and treatment group on OS. All analyses were conducted using the SAS System 9.2 (SAS Institute, Cary, NC, USA) for Windows.
RESULTS
Three-hundred forty-three patients were randomized: 172 to radical surgery and 171 to RT. Six patients were excluded from the analysis due to protocol violations, leaving 170 patients in the surgery arm and 167 in the RT arm who were included in the intention-to-treat analysis.
Ten patients crossed over treatment: 1 declined surgery and was irradiated, and 9 declined RT and therefore underwent surgery. These cases were analyzed according to the original group they were allocated to (intention to treat). Thus, 169 in the surgery group and 158 in the RT group underwent the scheduled treatment (compliance: 98% for surgery and 92% for RT). The flow of the patients into the trial is showed by the trial design (Fig. 1).
Fig. 1
Trial profile.
See original paper [1].
FIGO, International Federation of Gynecology and Obstetrics; RT, radiotherapy.

In the surgical arm, 9% of cases were stage IIA disease, 15% were adenocarcinoma, 32% had tumor diameter >4 cm and adjuvant RT was administered to 64% of the subjects (54% ≤4 cm, 84% >4 cm in diameter). In the RT arm, 13.7% (p=0.300) were stage IIA disease, 13% (p=0.400) were adenocarcinoma, and 34% (p=0.900) had tumor diameter >4 cm.
1. Survival and recurrence
The shortest follow-up is 19 years. No patient was lost to follow-up. Thirty-three patients (10%) died of intercurrent disease (31 cases) or fatal complications (2 cases).
Twenty-year OS is 72% and 77% for the surgical and RT arms, respectively (p=0.280; Fig. 2). When selected by tumor histology, OS for patients with squamous cell carcinoma is 72% for the RT arm and 82% for the surgery arm (p=0.040; Fig. 3A). If women with cervical size >3.5 cm are excluded, this difference is no longer significant with OS of 86% and 88% (p=0.990), respectively. Whereas beyond this cutoff survival differences between the 2 arms are clearly evident (Table 2). When selecting patients with adenocarcinoma histology, 20-year OS is 71% and 47% for surgery and RT (p=0.090; Fig. 3B), respectively. As a whole, 94 recurrences (28%) were observed. Median time to relapse was 13.5 (surgical arm) and 11.5 months (RT arm) (p=0.100).

Fig. 3
Overall survival for squamous cell carcinoma (A) and adenocarcinomas (B).
OP, surgery; RT, radiotherapy.

Table 2
Incremental survival differences in squamous cell carcinomas

| Cervical size (cm) | 20-year OS | p-value | ||
|---|---|---|---|---|
| No. of patients | Surgery (%) | RT (%) | ||
| ≤3.0 | 67 | 86 | 88 | 0.990 |
| 3.5 | 111 | 83 | 86 | 0.810 |
| 4.0 | 185 | 75 | 86 | 0.090 |
| 5.0 | 242 | 73 | 84 | 0.040 |
| Whole series | 287 | 72 | 82 | 0.040 |
After primary surgery 48 relapses (28%) were observed, 28 of them occurred in the pelvis. Five relapses after surgery (10%) were diagnosed beyond 5 years of follow-up (63–130 months). Post-surgical RT were administered to 75% of the relapsing cases. After primary RT 46 recurrences (27%) were recorded, 4 (9%) were diagnosed more than 5 years after irradiation (66–84 months). Thirty relapses occurred in the pelvis only. Eighteen patients (39%) presented with relapse within the cervix and underwent salvage surgery consisting of radical hysterectomy (14 patients) or anterior exenteration (4 patients), with a cure rate of 40% (12/30) for women with pelvic recurrence only.
Five patients who recurred after surgery (10%) and 15 after RT (33%) were salvaged. Details about the site of relapse are summarized in Table 3.
Table 3
Relapses by treatment modality

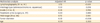
Multivariate analysis for OS confirms that significant risk factors for survival are histologic type (p=0.020), tumor diameter (p=0.008), and lymph node status (p<0.001) while treatment arm, age, histologic grade, and stage are not (Table 4).
Table 4
Multivariate analysis for survival
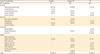
Complications after surgery were recorded in 32% of the patients (5 cases beyond 24 months). Five patients underwent surgery to treat their complications: 2 wound hernias, 1 ureteral fistula, 1 bowel obstruction and 1 peritonitis.
Complications in RT arm were observed in 23% of the patients (8 cases beyond 24 months). Four cases required surgical intervention to treat their complications: 1 abdominal hernia in a patient who had undergone surgery after external irradiation, 2 bowel obstructions and 1 ureteral stenosis.
The incidence of complications is significantly different between the 2 arms (p=0.006). Notably, hydroureteronephrosis was observed in 13 cases in the surgical arm, 11 (10.1%) of them diagnosed after surgery and adjuvant RT; all of them but 1 occurred within 24 months. Whereas in the RT arm, of the 9 cases of hydroureteronephrosis, only 5 (55%) occurred within 24 months. Moreover, leg edema occurred more often (11.1%) in the group of patients who received adjuvant RT after surgery as opposed to those who underwent radical hysterectomy with lymphadenectomy (none) or RT alone (0.6%). The same trend was observed for the incidence of bowel obstruction.
More details on morbidity according to the treatment groups are provided in Table 5.
Table 5
Complications related to the actual treatment
DISCUSSION
The publication of our randomized trial in 1997, of which results seemed to confirm the equivalence of radical surgery and RT for treating patients with stage IB–IIA cervical cancer, represents a firm milestone in the therapeutic management of these group of tumors. At least for squamous neoplasia cure rates were equal for the 2 treatment arms but the association of surgery and adjuvant RT worsened the associated morbidity. Such an outcome could be prevented by selecting patients prior to primary surgery on the basis of the cervical diameter in order to avoid the need for adjuvant treatment. Although our conclusion seemed clear and were supported by a high level of evidence, 3 other papers have been published since 2001 addressing the issue of optimal treatment for stage IB and IIA cervical disease (Table 1).
Brewster et al. [2] analyzed the Surveillance, Epidemiology, and End Results (SEER) 1995 database to select 1,039 women who received primary surgery (71%) or RT (29%). Patients with tumor diameter >4 cm were 26.6% and were unevenly distributed between the 2 groups (17% vs. 50%, respectively). The authors found a consistent survival advantage favoring surgery with respect to RT (5-year OS 84% vs. 69%, p<0.001). However, their analysis shows significant biases such as the greater percentage of women 40 years old or younger who underwent surgery instead of RT (82% vs. 18%, respectively). When subjects were stratified by tumor size, the younger cohort with tumors of 4 cm or less was more likely to be treated surgically than by RT (93% vs. 7%, respectively). Moreover, younger women with smaller cancers were significantly more likely to receive surgical treatment than their older counterparts (93% vs. 71%, p=0.001). Since the distribution of cervical size was not balanced and the younger patients were selected for primary surgery, it is not surprising that survival curves showed such a significant difference in favor of the surgical group. Furthermore, the analysis of that trial was based on an intent-to-treat design, with inclusion often of subjects into treatment groups that do not reflect the actual treatment received by patients in a given treatment category, adding confusion to its questionable results.
Bansal et al. [3] performed a similar analysis based SEER database updated to 2005. They extracted 4,885 patients who received surgery (4,012 cases) or RT (873 cases) as their first-line treatment. Even in this study, tumors greater than 4 cm in diameter are much more represented in the RT cohort (21% vs. 58%), as well as stage IIA (8% vs. 31%) and older age (p<0.001). Patients who were treated more recently were more likely to undergo surgery; whereas patients who were diagnosed before 1993 were more likely to receive primary radiation (p<0.001). Finally, 89.7% of patients with tumors ≤4 cm underwent surgery compared to 61.9% of patients with tumors >4 cm (p<0.001). Likewise, patients with IB1 tumors more commonly underwent surgery. Therefore, not surprisingly, performance of radical hysterectomy was associated with improved survival, and a 59% reduction in cancer-specific mortality.
Previous 2 studies considered respectively 152 women with stage IA to IIB neoplasia treated by radical surgery (115) or RT (37) and 198 stage patients with IB1 cancer treated by radical surgery (169) or primary by radiation therapy respectively (29) [45]. Five-year cancer-specific survival rates after primary surgery and after RT were comparable for the former (80% vs. 82%, respectively), whereas they were significantly different for the latter (95% and 70%, respectively). However, these studies are significantly biased by the small sample size and the poor study design.
In conclusion, all the above-mentioned trials are flawed by a remarkable patients' selection bias that prevents the drawing of a definitive conclusion as regards as a possible advantage of either treatment modality. Yamashita et al. [4] admitted that RT was preferred over surgery to treat elderly patients or women who were not medically fit to receive a surgical treatment. Doll et al. [5] as well stated that their patients in the radiation group were older (median age 47 years vs. 39 years, p=0.001), and had larger tumors (mean 3.0 cm vs. 1.5 cm, p=0.002). Similarly, in 2 larger studies analyzing SEER database the survival gain assigned to the surgical treatment seems to derive from an uneven selection of patients, since primary surgery was decided on the basis of the tumor diameter. This issue is more relevant when considering that patients with larger tumors, undergoing initial surgery, had increased chances of receiving postoperative RT, thus adding the morbidity of the 2 treatment modalities. Therefore, a cutoff of 3 cm has been already proposed as an appropriate criterion to select between surgery and RT as primary treatment since the Gynecologic Oncology Group study was published in 1990 [7].
Our long-term updated data confirm such an observation and show clearly that, at least for squamous tumors, surgical treatment has the same efficacy as RT only when the cervical size is no larger than 3 cm. In fact, for patients with cancers over 3.5 cm in size, RT yields better survival than surgery (Table 2). Conversely, primary surgery in patients with tumors >4 cm must be combined with adjuvant RT to yield acceptable survival rates, thus adding more frequent and worse morbidity than expected for each treatment alone as shown by the higher incidence of urologic complications such as ureteral stenosis and vascular complications such as lower extremities edema in patients receiving adjuvant treatment after radical hysterectomy.
Notwithstanding disease-free survival curves for surgery and RT arms are perfectly superimposed, whereas the 2 arms show different OS rates. The most likely explanation for such a difference is that many of the recurring patients after RT presented with a relapse localized either within the cervix or the proximal parametria, that could be cured in 40% of the cases by salvage surgery, while pelvic relapses after initial surgery (and adjuvant irradiation in most patients) were not cured in most cases. These findings strengthen the concept that women relapsing after receiving both treatments are hardly curable. However, we did not observe, after such a long follow-up, a significant difference in terms of incidence and pattern of recurrence in the 2 arms, as well as timing of relapse.
In our series about half of the patients with cervical cancers smaller than 4 cm and 84% of women with stage IB2–IIA2 tumors received adjuvant RT. According to these data, patients with squamous cervical cancers over 4 cm in size, and may be even over 3 cm, should not be treated with primary surgery. Interestingly a large analysis of the SEER database confirmed our findings since even within stage I tumors difference in tumor size between 3 and 4 cm represents a significant unfavorable prognostic factors for survival [8].
Another series confirmed the cut-off value of 2 cm has therapeutic and prognostic implications [9]. According to these and our results it appears reasonable to recommend primary surgery to patients with cancers smaller than 3 cm to minimize the risk of adjuvant RT.
In our present practice we follow the international guidelines for the treatment of cervical cancer and patients with squamous cervical cancers over 4 cm in size, and may be even over 3 cm if the stromal ring is involved, are not be treated with primary surgery but receive concomitant chemo-radiation treatment.
The introduction of neoadjuvant chemotherapy (especially cisplatin and paclitaxel based) prior to surgery has also contributed to reduce the need for postoperative radiation therapy to rates as low as 22% [1011]. Following these new therapeutic strategies, our current rate of adjuvant irradiation has lowered to 37.5%, reckoned over the last 10 years in 272 consecutive stage IB–IIA tumors operated since 2000. A reduced incidence of urologic (chronic hydronephrosis and atonic bladder) and vascular morbidity (lower extremities edema) represents the main benefit of this policy. On the contrary the incidence of such complications appear to remain higher when patients received both the 2 treatment modalities, with higher in cadence of ureteral stenosis, lower extremities edema and bowel obstruction.
Chances are that the introduction into the clinical practice of the modern irradiation techniques intensity-modulated radiation therapy (IMRT) may yield much better results both in terms of survival and morbidity with significant reductions in chronic gastrointestinal and urinary as well as vascular toxicities [12].
In the present study surgery was still confirmed as a better choice for patients with cervical adenocarcinoma regardless of the cervical diameter, since RT, at list in our hands, did not yields comparable survival results. In fact, we observed a significant difference in terms of survival between patients affected by squamous cell carcinoma as opposed to those with adenocarcinoma. In the literature there are studies that confirm adenocarcinoma histology as an independent risk factor for disease recurrence in patients with stage IB cervical cancer [16], as well as data that, in agreement with our own data, describe a better outcome of squamous cell carcinoma as opposed to adenocarcinoma when treated with RT only, whereas such a difference seems to have disappeared since chemo-radiation had been introduced as new standard of treatment [17].
In most recent years this issue was further evaluated by other studies that seem to confirm a reduced responsiveness of cervical adenocarcinoma to radiation [131415]. A Cochrane analysis in 2010 recommended surgery for early stage adenocarcinoma of the uterine cervix, primary chemo-radiation remains the second best alternative for patients unfit for surgery and it is probably the first choice in patients with magnetic resonance imaging (MRI) or positron emission tomography-computed tomography (PET-CT)-suspected lymph nodes involvement [18].
On the contrary for squamous histotype, as already mentioned, patients should be accurately selected for primary surgery, such as in case of cancer size not exceeding 3–4 cm, to minimize the need for adjuvant radiation treatment. Whereas alternative strategies such as preoperative chemotherapy or exclusive chemo-radiation should be undertaken to treat larger tumors or those with suspected parametrial involvement.
In conclusion the results of the present study seem to suggest that there is no treatment of choice for early stage cervical carcinoma in terms of survival. Long term follow-up confirms that the best treatment for the individual patient should take into account clinical factors such as menopausal status, comorbidities, histological type, and tumor diameter.
 XML Download
XML Download