

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In the treatment of vulvar high-grade squamous intraepithelial lesion (VHSIL) [1], cold knife, radiofrequency or laser excision, and vaporization may result in different degrees of disfiguring effects. In consideration of the risk of adverse somatic and psychosexual sequelae [234], less invasive treatments have been developed. These include photodynamic therapy and topical use of immunomodulators [23456].
In conservative treatments of VHSIL, it is of utmost importance to exclude the presence of foci of stromal invasion, which conveys an increased risk of metastatic spread to lymph nodes. If biopsy fails to detect the presence of invasive disease, the therapeutic approach and follow-up schedule may be suboptimal and survival rates will dramatically decrease [7]. By implication, biopsy should be directed—under vulvoscopic guidance—to the area at highest risk of invasion in order to obtain representative specimens for histologic evaluation [8910]. Vulvoscopy aims at detecting macroscopic changes in color, thickness and morphology of vulvar skin and mucosa. However, while cervical disease can be graded according to opacity, margins, contour, vasculature, and staining reactions of potentially abnormal epithelium, there is no grading system that helps differentiate vulvar lesions. This contributes to explaining why, in the clinical practice, the prevalence of clinically unrecognized stromal invasion in VHSIL varies up to over 20% of patients [811121314].
These problems call for a research effort to identify clues on how to decrease the risk that vulvoscopy-directed biopsy of VHSIL will fail to detect areas of invasive carcinoma. This involves identifying the patient and disease characteristics associated with stromal invasion, on which physicians could base their decisions for biopsy and subsequent treatment. Current knowledge about these characteristics is poor. Patient age is considered a risk factor, but the supporting evidence is circumstantial [15]. Moreover, no clinical risk factor has ever been identified [16].
The current article reports an analytical study of the prevalence and determinants of stromal invasion undetected at biopsy in a series of VHSIL patients from Italy.
MATERIALS AND METHODS
1. Setting
The study is part of a larger retrospective investigation of clinical presentation, diagnosis, treatment, and post-treatment outcomes of vulvar low-grade squamous intraepithelial lesion (VLSIL), VHSIL, differentiated-type vulvar intraepithelial neoplasia (dVIN), and invasive vulvar carcinoma at a tertiary-level referral center for vulvar disease in north-western Italy. All patients are seen on an outpatient basis. The policy for referral and admittance to the center has remained unchanged since its establishment in 1981.
2. Diagnosis and treatment
The examination of the vulva was performed under adequate lightening by naked eyes. A magnifying lens or a colposcope was used to better evaluate, if deemed necessary, the margins of lesions. Routine application of acetic acid was not used because of the previously reported high rate of false-positive results [10]. The clinical aspects of vulvar squamous intraepithelial lesion were described using the general principles of dermatology, defining location, focality, size, color, surface, thickness, and margination of the lesion [17]. Subsequently, in the most of suspicious areas, local anesthesia of the biopsy site was performed and a cold knife biopsy was taken. A standard diagram and digital images (when available) of the lesion were taken. Once the histological diagnosis of VHSIL was established, patients were submitted to excisional treatment. Biopsy and surgical specimens were processed according to a standard institutional procedure as previously described [1819].
Ten gynecologists, 6 pathologists, 3 dermatologists and hundreds of residents attended the center during the 35 years after its creation. In order to minimize the variability of clinical approaches, the diagnosis and treatment of all suspected cases of VHSIL and invasive carcinoma were only performed by 2 gynecologists (MP, LM), and all biopsy and surgical specimens were evaluated by 2 dedicated gynecologic pathologists (BG, SP).
3. Patients
The clinical and pathological records of patients histologically diagnosed with VLSIL, VHSIL, and dVIN between 1981 and 2014 were reviewed by trained personnel using a structured set of items of information. All available data were coded by the principal investigator. For patients with multiple diagnoses of vulvar squamous intraepithelial lesion, the index lesion was identified. Data from 302 consecutive patients were evaluated. Patients who were diagnosed with VLSIL (n=52) and dVIN (n=21), who refused treatment (n=7), and who received imiquimod as primary treatment (n=5) were excluded. There remained 216 eligible women.
4. Data analysis
Patient age was categorized into tertiles in order to detect a trend in the risk of unrecognized invasive carcinoma (if any) with the highest possible statistical power. The years of treatment were grouped into quartiles because of the unpredictable changes in disease care potentially associated with the long time span of the study. Lesion size was categorized in 2 groups only (<20 mm and ≥20 mm) in order to minimize the mismeasurement bias.
Differences in proportions were tested for significance with the chi-square tests for heterogeneity and trend, and the Fisher exact test. Differences in distributions were tested with the nonparametric Mann-Whitney test. Statistical significance was set at p<0.05. A p-value >0.05 and <0.10 was considered to indicate a borderline level of significance. Explanatory factors showing a statistically significant association with invasive carcinoma detection in univariate analysis were further examined in a multiple logistic regression model with backward stepwise selection of variables. The level of significance for removal of variables was set at p=0.10.
RESULTS
1. Patient characteristics
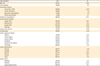
The yellow curve in Fig. 1 shows the frequency distribution of the 216 eligible patients according to 5-year age group. Although the pattern was not clearly bimodal, a peak was observed at age 40–44 years followed by a second frequency increase between 60–64 years and 70–74 years. Table 1 gives a summary overview of other major patient and disease characteristics. Noteworthily, more than 25% patients had an associated cervical intraepithelial neoplasia (CIN) and/or vaginal intraepithelial neoplasia (VAIN), and more than one third of lesions were multifocal.
Fig. 1
Frequency distribution of the 216 study patients according to 5-year age group and unrecognized invasive vulvar carcinoma detection at biopsy.

Table 1
Patient and disease characteristics of study cases of VHSIL
BMI, body mass index; CIN, cervical intraepithelial neoplasia; HIV, human immunodeficiency virus; VAIN, vaginal intraepithelial neoplasia; VHSIL, vulvar high-grade squamous intraepithelial lesion.
*Patients with missing information on each characteristic were excluded from the denominator; †Including lichen planus.
2. Prevalence of unrecognized invasive carcinoma
Invasive carcinoma unrecognized at biopsy was detected in surgical specimens from 24 patients (11.1%). The depth of stromal invasion varied between 0.1 mm and 3.0 mm with a median of 0.5 mm. In 4 of the 24 patients (16.7%), the depth of stromal invasion was >1.0 mm. The blue curve in Fig. 1 shows the frequency distribution of patients according to age group. Two peaks were observed at age 40–44 years and 70–74 years. Patients with unrecognized invasive carcinoma were older than patients free of invasion (median age, 64 vs. 48 years; p=0.005).
3. Risk factors for unrecognized invasive carcinoma
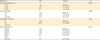
Table 2 shows the factors significantly associated with the prevalence of unrecognized invasive carcinoma in univariate analysis. The highest prevalence was observed in the subgroup of patients with involvement of 2 or 3 vulvar thirds (35.7%). Nonsignificant risk factors are listed in a footnote. A risk increase of borderline significance (p=0.072) was observed among VHSILs involving labia minora (16.5% vs. 6.8%).
Table 2
Significant univariate risk factors for clinically unrecognized invasive vulvar carcinoma detection in VHSIL (n=216)

The following were not significantly (p<0.05) associated with the prevalence of clinically unrecognized invasive carcinoma detection: BMI (<25, ≥25, unknown); comorbidity (no, human immunodeficiency virus positivity, other); associated cervical and/or vaginal intraepithelial neoplasia; associated lichen sclerosus, squamous hyperplasia, and other dermatoses; symptoms; involvement of labia majora, of labia minora, of vestibule, of posterior fourchette, and of perineum; whitish color; hyperpigmentation; unless otherwise indicated, variables were coded as: no, yes, unknown.
BMI, body mass index; VHSIL, vulvar high-grade squamous intraepithelial lesion.
*Test for trend.
Factors listed in Table 2 were examined further in a multiple logistic regression model, and 4 of them were demonstrated to be independently associated with the risk of invasive carcinoma detection in surgical specimens. As shown in Table 3, this was significantly increased for patients in the highest tertile of age, for patients with a lesion size ≥20 mm, and for patients with clitoral involvement. The risk increase for patients presenting with a nodular lesion was of borderline statistical significance. The univariate association of multifocality with the dependent variable was not confirmed by multivariate analysis.
Table 3
Significant multivariate risk factors for clinically unrecognized invasive vulvar carcinoma detection in VHSIL (n=216)
DISCUSSION
The finding of an unanticipated stromal invasion in a VHSIL confirms that the disease has a potential to progress [20] and that it is necessary to raise awareness about the limitations of vulvoscopy-directed biopsy in detecting early invasive carcinoma. Vulvoscopy serves two distinct functions: the estimation of severity of the lesion and the selection of biopsy site(s). Failure to ascertain the presence of stromal invasion may cause the patient to be undertreated and may have a strongly adverse impact on prognosis. In turn, this may lead the clinician to lose confidence in conservative treatments of VHSIL. According to previously reported case series, the biopsy site may be incorrectly selected in as many as 20% of patients [812]. The proportion was lower in our data, but it must be considered that our institution is a tertiary-level referral center for vulvar disease and that all diagnostic and treatment procedures were performed by the most experienced ones of us.
The rationale of this study is that an improved knowledge of the patient and disease characteristics associated with the presence of undetected foci of invasive carcinoma may assist the decision making for biopsy and treatment. First, in our data, the prevalence of stromal invasion increased regularly with increasing patient age, although a significant excess was demonstrated only when comparing the highest tertile of the variable with the lowest one. This observation is compatible with the univariate finding of van de Nieuwenhof et al. [21] that the risk of subsequent diagnosis of invasive vulvar carcinoma increases with the age at diagnosis of usual type vulvar intraepithelial neoplasia. Our observation also lends support to another previous study reporting an increased risk of invasive carcinoma detection among aged patients specifically presenting with a raised lesion [15]. It must be noted that our result was adjusted for the clinical features of VHSIL, which suggests that patient age predicts the presence of stromal invasion independently of these. In any case, we can confirm that excisional therapies are indicated for postmenopausal women [22].
The second key observation in this study was that the risk of unrecognized invasive carcinoma was greater among large-sized lesions. To interpret this finding, it should be noted that multivariate analysis did not confirm the causal role of multifocality that previous data had indirectly suggested [23]. We believe that lesion size is a confounder of the association between multifocality and the risk of invasive carcinoma detection. In other words, the univariate risk increase that is apparently due to multifocality is probably accounted for by the associated enlargement of the lesion, which indicates more rapid cell growth and spread and a greater amount of neoplastic epithelium at risk of progressing to invasive carcinoma. This hypothesis is in keeping with the evidence for a relationship between lesion size and disease recurrence [24].
The third, and most interesting, finding of this study was that the clitoral involvement conveyed a many-fold higher likelihood of clinically unrecognized stromal invasion. The incidence of invasive vulvar carcinoma with clitoral involvement has increased at a particularly rapid pace in recent decades, probably because the non-keratinized squamous cell epithelium covering the clitoris is less protected from human papillomavirus (HPV) infection [25]. In addition, the clitoral location of invasive vulvar carcinoma is associated with larger tumor size, deeper stromal invasion, and more frequent spread to lymph nodes. These unfavorable features have been related to patients' and physicians' delay in diagnosis [26], and this is a plausible explanation for our own observation. Patients' concerns regarding clitoral functionality and the hesitation to perform biopsies in order to avoid injury to the clitoral region do probably suggest a prolonged expectant management of VHSIL, with delayed diagnosis and clinically unrecognized disease progression. This attitude toward biopsy needs careful reflection. Although it is reasonable to balance the potential incremental benefit of taking a biopsy against functional and psychosexual contraindications, a more liberal biopsy of any suspicious areas is necessary to ascertain progression to invasive disease [3] and is especially indicated in patients undergoing an expectant management [9]. It is important that the peri-clitoral region be carefully inspected moving up the clitoral hood, so that the correct site for biopsy or biopsies be identified, and that the size of samples be adequate.
The risk of unrecognized invasive carcinoma detection was also found to be greater in nodular lesions, albeit at a weaker level of significance. An interesting analogy exists between this association and the well-documented clinical and prognostic significance of nodulation in pigmented skin lesions, in which this pattern of clinical presentation predicts rapid cell growth, local aggression, and vertical spread [27].
Among negative results, it is of note that human immunodeficiency virus (HIV) positivity did not predict the presence of invasive carcinoma. HIV-positive patients were more often diagnosed with unrecognized stromal invasion but not to a significant extent (2/14 or 14% vs. 22/202 or 11%, p=0.48, data not shown) and less than expected [28]. This was probably caused by their limited number and by the resulting random variability. In general, HIV-positive patients in the study area attend dedicated clinics.
There are several methodological issues in this study that need to be considered. First, we cannot completely rule out a selection bias in this single-institution case series. The prevalence of some patient characteristics differed from previous studies.
Second, the long time-span of patient accrual involves the risk that unpredictable time changes in disease behavior have introduced a bias in the results. Statistical adjustment for the year of diagnosis may be insufficient to control for this problem.
Third, the lack of information on patient HPV status is a limitation of the current study. Since HPV DNA is detectable in 87% patients with VIN vs. 29% patients with invasive vulvar carcinoma [29], it would be of interest to determine its prevalence among those VHSILs in which an early and clinically unrecognized stromal invasion has occurred. In the clinical practice, however, HPV DNA testing of specimens from VHSIL is not recommended [1]. In addition, during the first decade (1981–1990) of the study period, the specimens were fixed in Bouin's solution which prevents DNA analysis.
Last, but not less important, we wish to make a point on our treatment protocol. Since the risk of stromal invasion in patients with a biopsy diagnosis of VHSIL has always been a concern in our clinical practice, we have exceptionally used topical imiquimod (off-label use) as first line therapy, i.e., in 5 patients who have been excluded from this series. More often, although in selected patients, imiquimod has been used as adjuvant therapy after surgical excision. For the same reason, we do not use laser or radiofrequency vaporization of mucosal VHSIL in young patients. According to current practice guidelines [23], wide local excision is the treatment of choice if a patient with a biopsy diagnosis of VHSIL is suspected to have an occult cancer. In this study, we have considered the risk of clinically unsuspected stromal invasion, and we have identified some independent determinants. More data are needed before we can develop an appropriate statistical algorithm designed to predict the patient's individual risk. The ultimate objective is to personalize treatment based on the individual disease status, in order to avoid both under- and over-treatment.
We can conclude that patient age, lesion size and appearance, and clitoral involvement were independently associated with unrecognized invasive carcinoma detection. The clinical correlates of VHSIL progression and the accuracy of vulvoscopy in selecting biopsy sites warrant further investigations, possibly on a multicenter basis. In the interim, data currently available suggest that aged patients, patients with large and nodular lesions, and patients with clitoral involvement require special attention, with a timely, correct, and more liberal use of vulvar biopsy and the width of excision precisely tailored to the extent of disease.
 XML Download
XML Download