

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial carcinoma is the sixth most common malignant tumor worldwide, and there are approximately 290,000 new cases each year [1]. Because of its early clinical manifestations, such as postmenopausal or abnormal vaginal bleeding, the majority of patients are diagnosed at an early stage and have a favorable prognosis. The gold standard treatment is surgery along with hysterectomy and bilateral salpingo-oophorectomy (BSO), and comprehensive pelvic and para-aortic lymph node (PAN) dissection remains the standard of care in the staging of most endometrial cancers (EC).
Tumor grade, histological type, lymph node metastasis, depth of myometrial invasion and tumor size are known prognostic factors in EC. Based on these factors, EC has been defined to have low, intermediate or high risk. Depending on the prognostic factors, patients should avoid unnecessary adjuvant treatment and adopt more accurate surgical staging. Recently, lymphovascular space invasion (LVSI) was also an important prognostic factor for relapse of disease and poor survival.
LVSI includes lymphatic vessel invasion and blood vessel invasion, which were thought to be first stages of lymphogenous and hematogenous metastases, respectively. Interobserver variability in the evaluation of lymphatic and blood vessel invasion could not be neglected because of the difficulties in recognizing lymphatic channels and blood vessels using standard hematoxylin and eosin staining alone [2].
LVSI had been suggested to be an important prognostic factor for pelvic lymph node metastases in patients with EC [34]. For PAN, one study showed that para-aortic lymphadenectomy (PALND) in the majority of patients with intermediate risk or high-intermediate risk could improve their prognosis [5]. However, this type of surgery was associated with a higher cost and morbidity. Thus, some author suggested that PALND should not be used with patients with positive nodes, positive pelvic nodes, and >50% myometrial invasion as well as those who are LVSI positive. Patients without those clinicopathologic factors, they could avoid surgery [6]. Meanwhile, LVSI was suggested to be an independent risk factor in many cancers, such as cervical cancer [7], breast cancer [8] and colon cancer [9]. It was also shown that LVSI was strongly associated with lymph node (LN) metastasis in EC. Multivariate analysis confirmed LVSI (odds ratio [OR]=110.18; 95% confidence interval [CI]=38.43–315.87 [p<0.001]) as an independent predictor of lymphatic dissemination [10]. Another study showed that LVSI was an independent prognostic factor predicting PAN metastasis, and the sensitivity reached 97% [11]. Koskas et al. [12] also suggested that LVSI should be considered to be an independent risk factor for LN metastasis. On the other hand, Laufer et al. [13] found that LVSI and myometrial invasion had an independent association with tumor size (p<0.018). A tumor size greater than 2 cm was significantly and independently associated with LVSI and myometrial invasion among patients with early stage EC.
However, no study has covered preoperative factors predicting LVSI occurrence. It would provide very important information for the LN status. Therefore, the aim of this study was to establish a risk model for predicting positive LVSI among patients with EC before surgery. Knowing these risk factors would help gynecologists better adapt surgical staging and adjuvant therapies.
MATERIALS AND METHODS
1. Patients
This is a retrospective study that was approved by the Institutional Review Board of Shanghai First Maternity and Infant Hospital, Tongji University. Between January 2010 and March 2013, the medical documents of 211 patients with EC undergoing surgery were studied. They were divided into two groups based on positive LVSI and negative LVSI, and then, preoperative and postoperative pathological diagnoses were analyzed and compared to build a risk model for predicting LVSI.
2. Tissue samples
All patients underwent a total hysterectomy or radical hysterectomy with BSO and pelvic lymph node dissection. No radio-therapy or chemotherapy was administered before the operation. The specimens were reviewed by two gynecologic pathologists at the Department of Pathology in our hospital. A tumor was considered LVSI-positive when tumor emboli were noted within a space that was clearly lined by endothelial cells.
3. Data analysis
Data analyzed between two groups included the following variables: age, number of LN, total positive LN, white blood cell (WBC), CA19-9, CA125, carcinoembryonic antigen (CEA), fibrinogen (Fn), depth of myometrial invasion, International Federation of Gynecology and Obstetrics (FIGO) stage, tumor type (type I: estrogen-dependent; type II: estrogen-independent), tumor grade and cervical involvement. They were compared using χ2 tests. The results of the measurements were used to obtain receiver operating characteristic (ROC) curves for predicting LVSI. With the use of these curves, the threshold values of each variable were set. Logistic regression analysis was used to identify the possible risk factors for positive LVSI. Variables that achieved statistical significance in univariate analysis were subsequently included in a multivariate analysis.
The Statistical Package for the Social Sciences (Version 20.0; SPSS, Chicago, IL, USA) was used for all statistical analyses. A statistically significant difference was defined as a two-tailed p<0.05.
RESULTS
1. Patient characteristics
A total of 211 consenting patients with EC were entered in the study over the period from 2010 to 2013. Patients met the following criteria: 1) no tumor history, 2) no previous diagnosis of EC, and 3) no neoadjuvant chemotherapy or radiation therapy before examination or operation. The baseline characteristics of the 211 patients are presented in Tables 1 and 2.
Table 1
Baseline characteristics of the patients with EC

Table 2
Characteristics of the two groups
2. Analysis of pre- or post-operation factors between two groups
There were no differences in age, total positive LN, CA125, CA19-9, CEA, platelet (PLT) or tumor size between the positive LVSI and negative LVSI group, but the serum levels of Fn were higher in patients who had positive LVSI (p=0.024). LVSI-positive patients had a higher tumor grade (p=0.019), more tumors that invaded the outer-half of the myometrial invasion and a higher FIGO stage (p=0.000). Pelvic LN were more frequently invaded in patients with a positive LVSI (2/8) compared with patients with a negative LVSI (13/181, p=0.000). There was no significant difference for cervical involvement in patients with or without LVSI (p=0.065) (Table 3).
Table 3
Pathological findings post-surgery between the two groups
3. Receiver operating characteristic curves
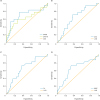
The expression of Fn and WBC before surgery in the LVSI positive and negative groups were significantly different. The ROC curves of the LVSI positive and negative groups were drawn with the use of Fn, CA19-9, CA125, CEA, and WBC values (Fig. 1). The curves obtained from the relationship between Fn and LVSI indicated a cutoff value of 2.58 with a sensitivity of 0.714 and a specificity of 0.635. The ROC curve also indicated that at the cutoff value of 21.2 U/mL, the variable CA125 had a sensitivity of 0.765 and a specificity of 0.694 in predicting LVSI. Similarly, the ROC curve revealed that at a cutoff value of 28.10 U/mL, the variable CA19-9 had a sensitivity of 0.588 and a specificity of 0.735 in predicting LVSI. The ROC curve showed that at a cutoff value of (6.35×109)/L, the variable WBC had a sensitivity of 0.714 and a specificity of 0.668 in predicting LVSI. The area under curve as 0.668 for Fn, 0.622 for CA19-9, 0.705 for CA125 and 0.648 for WBC.
Fig. 1
(A) ROC curve obtained from the relationship between CA125 or CA19-9 and LVSI. (B) ROC curve obtained from the relationship between CEA and LVSI. (C) ROC curve obtained from the relationship between Fn and LVSI. (D) ROC curve obtained from the relationship between WBC and LVSI.
ROC, receiver operating characteristic curves; LVSI, lymphovascular space invasion; CEA, carcinoembryonic antigen; WBC, white blood cell.
4. Analysis of factors related to LVSI in endometrial carcinogenesis
A χ2 test was used to analyze the factors, including Fn, CA19-9, CA125, CEA, and WBC, that were strongly associated with positive LVSI (p=0.000 for CA125, p=0.010 for CA19-9, p=0.002 for Fn, p=0.001 for WBC, and p=0.008 for CEA). The results showed that when CEA ≥1.84 U/mL, CA19-9 ≥28.1 U/mL, CA125 ≥21.2 U/mL and WBC ≥(6.35×109)/L, patients were more likely to have LVSI in our study (Table 4).
Table 4
Analysis of factors related to LVSI in EC
5. Logistic regression analysis
The multivariate logistic regression analysis in which LVSI was used as a dependent variable demonstrated that Fn (OR=2.751) and CA125 (OR=1.004) were associated with LVSI in EC. However, the final result identified only Fn (p=0.014) and CA125 (p=0.032) as cogent predictors of LVSI in EC (Table 5).

DISCUSSION
There has been much research on the relationship between LVSI and pathology in patients with EC. Through a multivariate analysis, Gadducci et al. [14] showed that LVSI was an independent predictive variable for the risk of distant hematogenous failure or recurrence. Patients with these pathological findings should be enrolled in randomized trials designed to assess the role of adjuvant chemotherapy alone or combined with sequential and/or concomitant external pelvic irradiation. Guntupalli et al. [15] identified 757 eligible patients, and 628 underwent systematic lymphadenectomy for staging purposes. In the multivariate analysis, progression free survival (PFS) and overall survival (OS) were significantly reduced in both LVSI positive groups (p<0.001) compared to patients who were LVSI negative. LVSI was highly associated with LN metastasis. This feature was useful in assessing the risk of metastatic disease and may serve as a surrogate for the prediction of extra uterine disease. A study by Vaizoglu et al. [16] found that lymphovascular space involvement was the sole predictor of lymph node metastasis in EC. Therefore, LVSI status should be requested from the pathologist during frozen examination whenever a decision to perform or omit lymphadenectomy is made. Thus, it was important to find factors to predict the risk of LVSI before the operation.
Our results showed that LVSI was related with myometrial invasion, tumor stage, tumor grade and histologic type. When the depth of myometrial invasion was more than 50%, LVSI was more likely. It was also observed that a higher tumor grade was associated with a higher rate of positive LVSI. Patients with LVSI were more prone to pelvic lymph node metastasis. However, the positive rate of LVSI in EC had no relationship with age. The occurrence of cervical involvement and LVSI had no significant correlation.
LVSI has been described as a predictor for nodal metastases or poor survival in ovarian cancer [17], vulva cancer [18], cervical cancer [1920], rectal cancer [21] and breast cancer [22]. Mariani et al. [3423] have published several studies with the objective of identifying new prognostic factors in EC. They and others have suggested that lymphovascular space involvement was an important prognostic factor for relapse of disease and poor survival. LVSI has also been shown to be an important prognostic factor for pelvic lymph node metastases in patients with EC [242526]. Therefore, we thought that predicting LVSI before surgery could help to better adapt surgical staging and adjuvant therapies.
Thus far, no specific serum tumor markers have been established for uterine endometrial carcinoma. It remains controversial whether the expression level of CA125 before surgery can predict lymph node metastasis in patients with EC. Takeda et al. [27] examined the preoperative serum CA125 levels in 64 patients with EC. There were five patients (7.8%) with pelvic or PAN metastases, but their serum CA125 was normal. There were 59 patients (92.2%) without nodal metastases, but there were eight lymph node-negative patients with preoperative serum CA125 levels above normal. Therefore, they thought that preoperative serum CA125 levels did not offer any information for predicting lymph node metastasis in patients with EC. However, an increasing number of studies have shown that the serum CA125 level was an independent risk factor for lymph node metastasis, which was the guide for whether a patient required LND [282930]. It has been reported that high CA125 values were associated with advanced surgical stage, lymph node metastasis, and poor prognosis [192021]. Another multivariate analysis using a logistic regression model showed that lymph node metastases had the most significant effect on the elevation of CA125 levels. The ROC curve determined that the best cutoff value was 40 U/mL; the sensitivity and specificity for screening lymph node metastases were found to be 77.8% and 81.0%, respectively. Therefore, they thought a CA125 level greater than 40 U/mL could be considered a criterion for full pelvic lymphadenectomy in the surgical staging of EC [30]. In our results section, the mean level of CA125 was 103.94 U/mL in LVSI-positive patients and 31.199 U/mL in the LVSI-negative group. The ROC curves showed that the cutoff value of CA125 was 21.1 U/mL with a sensitivity of 0.765 and a specificity of 0.694. The results of the logistic regression analysis revealed that CA125 was significantly related to LVSI in EC. Therefore, we thought that the expression level of CA125 could indicate the risk of LVSI in women with EC. It would guide more accurate surgical planning, such as lymphadenectomy and adjuvant therapies.
In this study, we were the first to show the relationship between fibrinogen and LVSI in EC. In patients with a malignant tumor, fibrinogen increase was associated with tumor metastasis, staging and prognosis. Fibrinogen had the highest concentrations of plasma coagulation factors is a thrombin and plasmin substrate. The development of gynecological malignancies due to tumor cell invasion and metastasis destroys a large amount of procoagulant substances in human blood, releases large amounts of tissue factors, and may start the clotting system. The formation of a large amount of thrombin fibrinogen was then converted to fibrous protein, thereby increasing the content of fibrin. Most solid tumors contain considerable amounts of fibrinogen-related products [3132]. Previously performed studies in mice lacking fibrinogen have demonstrated that loss of fibrinogen significantly diminishes the metastatic potential in breast cancer, lung carcinoma and malignant melanoma [33]. Seebacher, with 436 patients with EC within a retrospective multicenter study found that plasma fibrinogen levels can be used as an independent prognostic parameter for disease-free survival (DFS) and OS of patients with EC [34]. The research of Ghezzi et al. [35] found that the histological type, tumor grade, depth of myometrial invasion, surgical stage, patient age and hyperfibrinogenemia significantly affect DFS and OS rates. When these variables were entered simultaneously into a Cox regression model, increased preoperative levels of plasma fibrinogen retained significance as a predictor of poor DFS (OR=2.0; 95% CI=1.1–3.6) and OS (OR=2.7; 95% CI=1.3–5.5). Preoperative hyper-fibrinogenemia was an independent determinant of extrauterine disease (OR=2.7; 95% CI=1.3–5.6). In the sub-cohort of women with an endometrioid histology, an increased fibrinogen concentration at presentation was predictive of pelvic nodal involvement (OR=3.6; 95% CI=1.1–11.7). The plasma fibrinogen level may be an independent risk factor in EC [35]. Palumbo has already studied a mouse model and found a lack of Fn in mouse lymph and hematogenous metastasis [36]. In our results, the mean level of Fn was 2.78 U/mL in LVSI-positive patients and 2.49 U/mL in the LVSI-negative group. The difference was statistically significant. The ROC curves showed a cutoff value of Fn of 2.58 U/mL with a sensitivity of 0.714 and a specificity of 0.644. The logistic regression analysis revealed that the expression level of Fn was significantly related to LVSI in EC. We found that we could predict the occurrence of LVSI in endometrial carcinoma.
In summary, we wanted to combine CA125 with fibrinogen to build a model to predict the risk of LVSI in women with EC. Our study showed that a serum level of CA125 ≥21.1 U/mL and an Fn ≥2.78 U/mL are promising factors for the prediction of LVSI in EC. If the present findings are replicated in future studies, the determination of the plasma fibrinogen and CA125 levels may help to obtain a more precise individual risk profile for LVSI in EC. It should be noted that detecting the serum levels of CA125 and Fn in patients with EC may guide more accurate surgical planning, such as for lymphadenectomy and follow-up adjuvant therapies. This process may improve the prognosis or quality of life in patients with EC.
 XML Download
XML Download