

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tamoxifen is widely used for the postoperative endocrine treatment for both pre- and postmenopausal patients with estrogen receptor (ER)-positive breast cancer [1]. Tamoxifen is known to be a selective estrogen receptor modulator (SERM), which acts as an ER agonist or antagonist according the type of tissue [2]. For example, tamoxifen exhibits competitive receptor inhibition in the breast tissue, however, it also demonstrates partial nonsteroidal agonistic activity in bone and endometrium [1]. Therefore, tamoxifen users can experience several adverse events, including vasomotor symptoms, the occurrence of ovarian cyst(s) and the increased risk of endometrial hyperplasia or cancer [34].
Furthermore, tamoxifen can affect menstruation and its range was reported from no effect on menses to complete cessation of menstruation [5]. Although the mechanism of amenorrhea is not well understood, it may be resulted from the increased plasma level of estrogen and the interference with hypothalamus-pituitary-ovarian axis [567]. The prevalence of amenorrhea or severe oligomenorrhea was reported as –65% in a previous study [6] and amenorrhea was experienced in as high as 61% of patients [8].
In patients undergoing tamoxifen treatment, amenorrhea can be explained by the effects of tamoxifen. However, the evaluation of amenorrhea in these patients should begin with thorough medical history, physical examination and laboratory tests, etc. If amenorrheic patients have no relevant history of abnormal genital tract abnormality, further stepwise evaluation is needed to diagnose the etiology of amenorrhea and the ovarian and pituitary dysfunction is one of the most commonly encountered cause of amenorrhea [9]. However, the endocrine evaluation seems to be omitted in the patients with tamoxifen treatment [7] and few studies have demonstrated the hormone profile in this population. This study aimed to investigate whether the ovarian and pituitary function lies within a normal range in the amenorrheic patients taking tamoxifen for the prevention of recurrence of breast cancer.
MATERIALS AND METHODS
1. Subjects
The study population consisted of fifty-nine premenopausal breast cancer patients whose stage of breast cancer was restricted to stage 0 (e.g. ductal carcinoma in situ). They were referred to the Department of Obstetrics and Gynecology at Seoul National University Hospital and all of the participants underwent gynecologic surveillance during tamoxifen treatment (20 mg/day). The menstrual history and gynecologic information, including the number of pregnancy and live birth, was reviewed from the medical records. Amenorrhea was calculated in months and it was defined as the absence of menstruation for a time equal to a total of three previous cycles since the previous menstrual period. Those who had a previous history of chemotherapy or serum follicle stimulating hormone (FSH) concentrations equal to or higher than 30 mIU/mL were excluded since they were at menopausal transition. Those who received aromatase inhibitor, herceptin or gonadotropin releasing hormone (GnRH) agonist treatment were also excluded. All clinical information was collected and retrospectively reviewed. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital.
2. Measurement of serum hormones, tumor markers and endometrial thickness
Serum hormones were measured between cycle days 2 and 5 in patients with menstruation or at any time in amenorrheic participants. Serum luteinizing hormone (LH) and FSH were determined with immunoradiometric assay kits (Siemens Healthcare Diagnostics Inc., Deerfield, IL, USA). Serum estradiol was measured using a radioimmunoassay kit (Siemens Healthcare Diagnostics Inc.), and minimal detection limits were 8 pg/mL. Immunoradiometric assay kits (DiaSorin, Saluggia, Italy; ShinJin Medics Inc., Goyang, Korea) were used to determine the levels of thyroid stimulating hormone (TSH) and prolactin.
Serum carcinoembryonic antigen (CEA) and cancer antigen 15-3 (CA 15-3) were measured using non-competitive immunoradiometric assay kits (ShinJin Medics Inc.) and solid-phase sandwich immunoradiometric assay kits (Cisbio Bioassays, Coldolet, France) with minimal detection limits of 0.18 ng/mL and 0.2 U/mL, respectively.
During the gynecologic examination, transvaginal ultrasound was performed to detect uterine and ovarian abnormalities using an ultrasound system with a transvaginal probe of 5.0 MHz (Medison, Seoul, Korea). The endometrial thickness (EM thickness) was measured as the width of the anterior and posterior layer of the endometrium in the sagittal plane of the uterus.
3. Immunohistochemical staining
Immunohistochemical (IHC) staining was conducted in regard to estrogen receptor (ER) (1:100, 1D5; Dako, Glostrup, Denmark), progesterone receptor (PR) (1:200, PgR636; Dako), B-cell lymphoma 2 (Bcl-2) (1:200, 124; Dako), Ki-67 (1:300, MIB-1; Dako), epidermal growth factor receptor (EGFR) (1:100; Zymed, San Francisco, CA, USA), and human epidermal growth factor receptor 2 (HER2) (1:200, CB11; Leica Microsystems, Berlin, Germany) on the cut sections of specimens. Positive staining was defined as nuclear staining in ≥1% of the tumor cells for ER and PR. For Bcl-2, cytoplasmic staining in ≥10% of the tumor cells was defined as positive. The Ki-67 proliferation index of each case was evaluated from the percentage of Ki-67-positive cells among at least 200 tumor cells. Only the membranous staining of tumor cells was scored for the determination of HER2 expression, and the intensity was scored as follows: 0 for negative staining, 1+ for weak staining, 2+ for moderate staining, and 3+ for strong staining in at least 30% of the tumor cells.
4. Statistical analysis
All data were expressed as mean±standard deviation or number of participants. All statistical analyses were performed using the Statistical Package for Social Science 21.0 (SPSS Inc., Chicago, IL, USA). The data were analyzed with the Student t-test, χ2 test and Fisher’s exact test. The p value of less than 0.05 was considered to be significant for all analyses.
RESULTS
1. Baseline characteristics according to the presence of menstruation
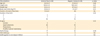
A total of 59 premenopausal tamoxifen users were identified for analysis and the overall prevalence of amenorrhea was 61.0% (36/59) (Table 1). The duration of amenorrhea was 10.2 months and mean age of amenorrheic women was comparable to that of women with regular menstruation (42.3±5.3 vs. 41.6±4.0 years). No significant differences were observed in regard to the body habitus, obstetric history, previous menstrual regularity and mode of treatments between the two groups. Menstrual intervals were 26.8±2.6 vs. 27.8±3.0 days (regular menses vs. amenorrhea); the duration of tamoxifen use 24.5±4.7 vs. 23.7±4.4 months. The onset time of amenorrhea from the initiation of tamoxifen was 22.4±3.6 months. The study groups were followed for 39–55 months after breast cancer surgery and tamoxifen was started from within one month after surgery during this follow-up period.
Table 1
Baseline characteristics according to the presence of menstruation in premenopausal tamoxifen users
2. Immunohistochemical marker positivity according to the presence of menstruation
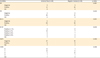
IHC marker positivity of surgical specimen was compared between the two groups. The compared variables included ER, PR, Bcl-2, Ki-67, EGFR and HER2. None of the compared markers showed any significant difference according to the presence of menstruation (Table 2). No correlation was observed between IHC results and hormone profiles, however, amenorrheic group showed a higher prevalence of HER2 0 and HER2 1+ when compared to regular menses group (p=0.006).
Table 2
Immunohistochemical marker positivity according to the presence of menstruation in premenopausal tamoxifen users
3. Serum level of hormones and tumor markers according to the presence of menstruation
Amenorrheic women had a significantly higher level of serum FSH than that of women with regular menses (8.1±5.7 vs. 5.1±2.2 mIU/mL, p=0.01), which may suggest decreased ovarian reserve (Table 3). Regularly menstruating women demonstrated significantly increased EM thickness compared to that of amenorrheic group (7.4±4.1 vs. 5.4±2.3 mm, p=0.04), suggesting increased serum estrogen concentrations, however the difference of estrogen levels did not reach a statistical significance. Serum TSH level was significantly lower in amenorrheic group (p=0.04), although the mean values of both groups were within a normal range (Table 3). The distribution of serum TSH and prolactin level were not different according to the presence of menstruation (Table 4).
Table 3
Serum level of hormones and tumor markers according to the presence of menstruation in premenopausal tamoxifen users

Table 4
The distribution of serum TSH and prolactin according to the presence of menstruation in premenopausal tamoxifen users

DISCUSSION
Amenorrhea is defined as the absence of menstruation for a time equal to a total of three previous cycles or 6 months in women with previous normal menses [9]. It has been suggested to investigate the underlying causes if menstruation is delayed for three months or longer [10]. Although the prevalence of amenorrhea, not caused by pregnancy, lactation or menopause, has been reported up to 3%–4% [1112], it is one of the most commonly presented symptoms in women with breast cancer. Approximately 60%–84% of patients has been reported to experience amenorrhea after chemotherapy [1314] and the prevalence differed according to the chemotherapeutic regimen.
Tamoxifen seems to have an additive effect on the prevalence of amenorrhea since a significantly greater number of patients have experienced amenorrhea after chemotherapy and tamoxifen, compared to those who received chemotherapy only. Considering that chemotherapy can induce ovarian suppression for a considerable duration, the effects of tamoxifen on the menstrual function should be assessed in patients who did not receive chemotherapy. For this reason, in the present study, the patients with previous history of chemotherapy were excluded. The prevalence of amenorrhea in this study was 61% and it is comparable to the previous study in which severe oligomenorrhea and amenorrhea was reported in up to 65% of the participants [6].
The FSH concentration during early follicular phase is widely used for the test of ovarian reserve [9]. The women with serum FSH level equal to or higher than 30 mIU/mL were not included in this study since a high level of FSH indicates decreased ovarian reserve or impending ovarian failure. In the present study, amenorrheic women demonstrated a significantly higher FSH level as in the case of normal tamoxifen-nonuser population. In contrast, Berliere et al. [6] reported that the FSH levels are 20 (6–25) mIU/mL vs. 1.1 (0.5–20.7) mIU/mL (regular menses vs. amenorrhea). Differences in values between that and ours may have been resulted from different sample size and ethnicity. However, cautious interpretation is needed since the Belgian study represent median values while ours are mean values. Recently, anti mullerian hormone (AMH) has been frequently measured at many infertility clinics since its higher correlation with ovarian reserve and less menstrual cycle-dependent variation compared to FSH. However, due to the insurance coverage issue at our breast cancer clinic, AMH has not been measured routinely.
Serum estradiol level is another reproductive aging marker and it is secreted from the ovary during follicular development. An elevated level (greater than 60–80 pg/mL) at cycle days 2–4 of menstrual cycle may indicate decreased ovarian reserve and may precede the elevation of FSH levels [1516]. In the present study, serum estradiol levels were not statistically different according to the menstruation status, although women with regular menses tended to have a higher estradiol level and this finding may explain greater EM thickness in these women. Intriguingly, in a previous report, patients who continued to menstruate during tamoxifen treatment demonstrated supraphysiologic estradiol levels [17].
It has been suggested that tamoxifen may induce changes in hypothalamus-pituitary axis [18]. Hyperprolactinemia is one of the easily identified disorders of anovulation and amenorrhea and, although less common, thyroid diseases are the other common causes of anovulation. Therefore, measurement of serum prolactin and TSH level is strongly recommended in all women with amenorrhea [9]. In this study, hyperprolactinemia was found in six patients, however, the prolactin level was only minimally elevated with the range of 22.0–34.1 ng/mL and sella MRI was not performed. Currently, little is known in regard to the prevalence of hyperprolactinemia in tamoxifen users, although some researchers provided the evidence that tamoxifen alters the prolactin levels [19].
Serum TSH level was significant lower in amenorrheic women and the prevalence of low TSH level was 8.3% in the present study. The clinical significance of different TSH levels between the two groups is not clear since they lie within euthyroid ranges. However, our data may provide clinicians with an insight that tamoxifen-induced subclinical alteration in thyroid function should be monitored in those taking this mediation.
Tamoxifen has been reported to reduce thyroxine binding globulin (TBG) clearance through binding to a protein with heavier glycoside [20]. Indeed, a previous study showed an increase in thyroxine uptake and TBG levels at three months after tamoxifen use [21]. To the best of our knowledge, this is the first study that analyzed thyroid function in amenorrheic women taking tamoxifen use.
Taken together, our results, i.e. FSH elevation and TSH decrease, may provide an insight over any possible subclinical alteration of the pituitary hormone levels in amenorrheic, post-operative tamoxifen users. This issue is important and should be adequately addressed during the gynecological counseling of referred breast cancer patients.
Interestingly enough, amenorrheic group showed a higher incidence of HER2 0 and HER2 1+ compared with regular menses group, although no correlation was observed between IHC results and hormone profiles. Fluctuation of HER2 expression in breast carcinomas during the menstrual cycle was reported [22], however, the influence of this fluctuation on the endometrial tissue is not clear at present.
In this study, many markers such as CEA and CA 15-3, EGFR, Bcl-2, and Ki-67 were examined to find any correlation with endocrine variables as in the previous report. Han et al. [8] reported that E2 levels were positively correlated with serum CA 15-3 in the subgroup analysis. However, no significant correlation between hormone levels and tumor markers was found in this study population.
The present study has a few limitations and should be interpreted with a caution. First, a relatively small number of breast cancer patients were included in the present study and it might decrease the power of the study. A larger prospective study seems to be needed due to the cross-sectional feature and small sample size of the present study. Second, tamoxifen use may be a confounder in the analysis of serum FSH and estradiol concentrations as described previously.
In conclusion, menstruation status and hormone levels may be influenced by tamoxifen use in premenopausal breast cancer patients. Physicians should be attentive to the alteration of pituitary hormone levels in addition to sex steroid hormones in this population. Individualized counseling and quality of life care should be considered in this population. Further larger-scale, prospective investigation is needed to confirm our data and to elucidate the underlying mechanisms.
 XML Download
XML Download