

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine cervical cancer is one of the most common malignancies in women worldwide. In the United States, an estimated 12,900 new cases are expected to be diagnosed and 4,100 women are expected to die of cervical cancer in 2015 [1]. Bone metastases are a frequent complication of cancer, occurring in up to 70% of patients with advanced breast or prostate cancer [2]. In contrast, being generally uncommon in cervical cancer and thus, there has been limited information of bone metastasis as a prognostic factor [34567]. Some reports showed that >60% of cervical cancer patients died within 6 months of being diagnosed with a bone metastasis [34]. Other reports showed median survival time of 7 to 12 months for cervical cancer patients after diagnosis of a bone metastasis [567]. For patients with bone metastasis, prediction of their remaining weeks or months might be important with regard to treatment decisions and quality of life.
Katagiri et al. [8] conducted a prospective study based on data of their cohort of 350 cases comprising various primary tumors and proposed a scoring system to estimate the prognosis of patients with bone metastasis. They identified five significant prognostic factors: (1) site of the primary lesion; (2) presence of visceral or cerebral metastases; (3) performance status (Eastern Cooperative Oncology Group [ECOG] status 3 or 4); (4) any previous chemotherapy; and (5) multiple bone metastases. Moreover, they proposed a new scoring system incorporating another factor, abnormal laboratory data, based on data of their cohort of 808 cases [9]. Every case was scored from 0 to 10, calculated by adding all individual factors. Survival rates were 98.1%, 74.0%, and 26.9% at 6 months, and 91.4%, 49.3%, and 6.0% at 1 year in patients with scores of 0 to 3, 4 to 6, and 7 to 10, respectively. However, it is unclear whether these results are applicable because there were only nine cases (1.1%) of cervical cancer in their study population. In their scoring system, cervical cancer was classified in the rapid growth group, which included hepatocellular, gastric, and lung carcinomas. We evaluated biological aggressiveness of bone metastasis peculiar to cervical cancer and verified each prognostic factor selected in the Katagiri et al. [89] study. A prognostic scoring system particular to bone metastasis from cervical cancer was proposed in this study.
MATERIALS AND METHODS
1. Patients
In total, 925 patients were treated for cervical cancer at the National Hospital Organization, Hokkaido Cancer Center from January 1995 to December 2014. Fifty-four patients (5.8%) with skeletal metastasis from cervical cancer were included in the study. The medical records were reviewed, and data at the time of initial presentation, which included age, International Federation of Gynecology and Obstetrics (FIGO) stage, histological subtype, and treatment, were collected. Data at the time of initial progression, namely the progression-free interval, were also investigated. In addition, data at the time of bone metastasis diagnosis, which included spread pattern, presence of extraskeletal metastasis, performance status (evaluated according to the ECOG performance status group [10]), history of any previous radiation or chemotherapy, number of bone metastases, onset time and treatment, were collected. Finally, data regarding clinical outcome were obtained. The local Institutional Review Board and the hospital's Ethics Committee approved the study protocol.
2. Diagnosis of bone or extraskeletal metastases
The presence of bone or extraskeletal metastases was determined by biopsy or imaging including bone scans, fluorodeoxyglucose-positron emission tomography, computed tomography, and magnetic resonance imaging. Radiologically abnormal lesions without pathological confirmation found in patients diagnosed with other types of invasive cancer within the previous 5 years were not considered as metastatic tumors. The metastatic status of bone lesions that appeared to be in a gray zone was determined by specialists in orthopedic oncology.
3. Survival analysis
The primary outcome measure was the survival period after diagnosis of bone metastasis. Eight variables were used for survival analysis and every variable had a binary classification. (1) Histological variant (squamous cell carcinoma vs. non-squamous cell carcinoma); (2) spread pattern (direct invasion from primary tumor or metastatic tumor vs. hematogenous spread); (3) extraskeletal metastasis (no vs. yes); (4) performance status (0 to 2 vs. 3 to 4); (5) history of any previous radiation or chemotherapy (no vs. yes); (6) multiple bone metastases (no vs. yes); (7) progression-free interval (≥12 months vs. <12 months); and (8) bone metastasis-free interval (≥12 months vs. <12 months). Skeletal lesions without abnormal imaging findings in the adjacent soft tissues were classified as hematogenous metastases. Previous radiation included all types of radiation therapy including definitive or palliative radiation for primary or metastatic tumors.
Progression-free interval was defined as the time from initial presentation to initial progression or death from any cause, which did not depend on the presence or absence of bone metastasis. The bone metastasis-free interval was defined as the time from initial presentation to diagnosis of bone metastasis from cervical cancer. Survival rates were estimated using the Kaplan-Meier method and compared between groups using the log-rank test. Hazard ratios (HRs) and 95% CIs were estimated using the Cox proportional hazards model. A p<0.05 was considered statistically significant. All analyses were performed using StatView-J ver. 5.0 (SAS Institute, Cary, NC, USA).
RESULTS
Clinicopathological characteristics of the 54 patients are shown in Table 1. A total of nine patients (16.7%) had FIGO (2008) stage I disease, 12 (22.2%) had stage II disease, 12 (22.2%) had stage III disease, and 21 (38.9%) had stage IV disease. Forty-two patients (77.8%) had squamous cell carcinomas. Treatment of primary cervical tumors involved radical surgery followed by radiation or chemotherapy in 10 patients (18.5%). Concurrent chemoradiotherapy was given to eight (14.8%), and eight (14.8%) were given chemotherapy followed by radiotherapy.
Table 1
Profile of patients at the time of initial treatment (n=54)

CCRT, concurrent chemoradiotherapy; CT, chemotherapy; FIGO, International Federation of Gynecology and Obstetrics; RT, radiation.
![]()
Clinical characteristics of the bone metastases are shown in Table 2. Bone metastasis occurred by hematogenous spread in >80% of cases. Fifty patients (92.6%) had extraskeletal metastasis at the time of diagnosis of bone metastasis. Twenty-eight patients (51.9%) had a performance status ≥3. Thirty-nine patients (72.2%) had a history of receiving previous radiation or chemotherapy. Thirty-three patients (61.1%) had multiple bone metastases. Approximately a quarter of bone metastases occurred at the time of initial presentation, another 25% occurred at the time of initial progression, and the remaining half occurred at the subsequent progression.
Table 2
Clinical characteristics of bone metastasis (n=54)

CT, chemotherapy; ECOG, Eastern Cooperative Oncology Group; RT, radiation.
*Bone scans, fluorodeoxyglucose-positron emission tomography, computed tomography, and magnetic resonance imaging.
![]()
As for treatment of the metastatic bone tumor, radiotherapy alone was done in 53.8% of cases. Best supportive care was performed in 18.5% of patients. Spinal fixation was performed in three (5.6%) of the patients.
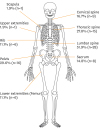
As shown in Fig. 1, bone metastasis to the vertebral column was usual. The most common site of bone metastasis was the lumbar spine (51.9%), followed by pelvis (29.6%), thoracic spine (27.8%), cervical spine (16.7%), and sacrum (14.8%).
The Kaplan-Meier curve for the entire cohort is shown in Fig. 2A. The median survival period after diagnosis of bone metastasis was 22 weeks (range, 2 to 207 weeks). The overall rate of survival after diagnosis of bone metastasis of the entire cohort was 64.2% at 13 weeks, 37.2% at 26 weeks, and 15.7% at 52 weeks.
 | Fig. 2Kaplan-Meier survival curves after diagnosis of bone metastasis in all 54 patients included in this study (A) and in patients with prognostic scores of 0 to 1, 2, 3, and 4 to 5 (B). The rates of survival for these four groups were significantly different (p<0.001).
|
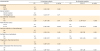
Table 3 shows the results of Cox regression analysis of prognostic factors in cervical cancer patients with bone metastasis. The following five factors were confirmed as independent prognostic factors in a multivariate analysis: (1) extraskeletal metastasis (HR, 6.1; 95% CI, 2.2 to 16.6); (2) performance status of 3 to 4 (HR, 7.8; 95% CI, 3.3 to 18.2); (3) previous radiation or chemotherapy (HR, 3.3; 95% CI, 1.4 to 7.8); (4) multiple bone metastases (HR, 1.9; 95% CI, 1.0 to 3.5); (5) bone metastasis-free interval of <12 months (HR, 2.5; 95% CI, 1.2 to 5.3). A prognostic score was calculated by adding up the number of significant factors and therefore, every case was scored from 0 to 5.
Table 3
Prognostic factors for the survival period after diagnosis of bone metastasis selected using Cox proportional hazards model analysis
![]()
Table 4 shows survival rates according to this scoring system. None had a score of 0 and only three (5.6%) had a score of 1. Each of these survived 17, 20, and 27 months after diagnosis of bone metastasis, respectively. The median survival periods after diagnosis of bone metastasis was 84 weeks for those with a score ≤1, 33 weeks for those with a score of 2, 25 weeks for those with a score of 3, and 13 weeks for those with a score ≥4. The rates of survival for these four subgroups were significantly different (log-rank test, p<0.001) (Fig. 2B). The 13-week survival rates after diagnosis of bone metastasis were 90.9% for those with a score of 2, 81.3% for those with a score of 3, and 37.5% for those with a score ≥4. The 26-week survival rates were 61.4% for those with a score of 2, 43.8% for those with a score of 3, and 12.5% for those with a score ≥4. The 52-week survival rates were 40.9% for those with a score of 2, 6.3% for those with a score of 3, and 0% for those with a score of ≥4.

DISCUSSION
The present study showed a median survival time of 5 months for patients with bone metastasis from cervical cancer, which is consistent with results of some earlier studies [34], despite others showing median survival times of ≥7 months [567]. Indeed, only two patients (3.7%) in our cohort survived more than 2 years. In the scoring system proposed by Katagiri et al. [89], cervical cancer was classified in the rapid growth group, which included hepatocellular, gastric, and lung carcinomas. Our result concurred with their classification regarding biological aggressiveness of bone metastasis from cervical cancer. For such patients, prediction of their remaining lifespan would allow them to better plan how to live out their final days. There are some options including surgery for the treatment of bone metastasis. Life expectancy of at least two months is usually required before surgery is considered for metastases to the limbs [11], and of three to six months for metastases to the spine [1213]. According to our results, patients with a prognostic score of ≤1 were very good candidates for spinal surgery. However, this group accounted for only 5.6% of the entire cohort. Patients with a prognostic score of 2 might also be good candidates for spinal surgery. Of 11 patients with a prognostic score of 2, seven had any one of cervical, thoracic, or lumbar spine metastases, which accounted for only 13.0% of the entire cohort. Cases of metastases to the spine, for which surgery was the preferred treatment, amounted to only 20% or less of patients with bone metastasis from cervical cancer.
Katagiri et al. [89] identified five significant prognostic factors: (1) site of primary lesion; (2) presence of visceral or cerebral metastases; (3) performance status; (4) any previous chemotherapy; and (5) multiple bone metastases. On the other hand, Kanayama et al. [7] showed that the bone metastasis-free interval was a significant predictor of survival period. All above-mentioned factors independently functioned as significant predictors of survival in the present study; thereby, confirming the reproducibility of results in previous ones. A history of previous radiation or chemotherapy and time to onset (i.e., initial presentation vs. initial or subsequent progression) might have had a combined effect that confounded the analysis. When we included the onset time along with the five significant prognostic factors in the multivariate analysis, five variables were confirmed as independent prognostic factors. These were (1) extraskeletal metastasis (HR, 6.8; 95% CI, 2.4 to 18.7); (2) performance status 3 to 4 (HR, 9.2; 95% CI, 3.8 to 22.2); (3) multiple bone metastases (HR, 2.0; 95% CI, 1.1 to 3.6); (4) bone metastasis-free interval of <12 months (HR, 3.0; 95% CI, 1.4 to 6.3); and (5) onset time at initial presentation (HR, 0.2; 95% CI, 0.09 to 0.5). A history of previous radiation or chemotherapy was not found to be an independent prognostic factor. We found a significant association between previous chemotherapy and a poorer prognosis (adjusted HR, 2.7; 95% CI, 1.2 to 6.3) after adjusting for extraskeletal metastasis, performance status, multiple bone metastases, and bone metastasis-free interval. Treatment-related factors for bone metastasis were not included in our survival analysis. However, treatment-related factors were unlikely to have influenced our results because there have been no effective drugs that have achieved long-term survival in recurrent cervical cancer patients. The objective of treatment for patients with bone metastasis from cervical cancer is usually symptom palliation.
Our study has some limitations. First, the number of patients included in the study was too small to power statistically conclusive results. Second, there was no consistent follow-up policy for diagnosing metastatic bone tumors, and no consistent treatment policy for patients with metastatic bone tumors in our institution. These issues were caused by the fact that ours was a retrospective, observational study conducted at a single institution. Third, impact of each factor on prognosis might differ according to its characteristics. Each five prognostic factor was given equally one point as a score in our scoring system; thus, there is still room for improvement in our scoring system.
However, ours was a validation study to confirm the results of a larger, prospective study [89]. Our finding, in which all previously reported factors were confirmed as prognostic factors in a small-sized cohort, should be considered significant. In addition, our institution is a tertiary cancer center with a division of orthopedic oncology, radiation oncology, and palliative care. Insufficiency fractures or compression fractures were appropriately excluded from our study by physicians who were in charge of orthopedic oncology. Many patients with metastatic bone tumors are referred to our institution in a state in which the primary tumor is unknown. Many patients already treated with standard therapy are referred to our institution for the purpose of palliative treatment including radiation therapy in the latter half of their clinical course. These additional factors also lend support to the validity of our study.
In conclusion, classifying cases of bone metastasis from cervical cancer as a rapid growth group is appropriate. Extraskeletal metastasis, performance status, previous radiation or chemotherapy, multiple bone metastases and bone metastasis-free interval might be independent prognostic factors for patients with bone metastasis from cervical cancer. Our scoring system based on these five factors can be used to determine the optimal treatment for patients with bone metastasis from cervical cancer.
 XML Download
XML Download