

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is still the fourth most common women's cancer death in the world; however, early detection of high grade cervical intraepithelial neoplasia (CIN) enables patients to receive conservative treatment [1]. Conization is widely accepted as the standard method of conservative treatment for CIN. Persistent or recurrent disease after conization, however, was observed in approximately 5.5% to 31.6% of patients [23456]. Several variables such as older age [2], multiparity [3], high CIN grade [4], posttreatment human papillomavirus infection [5], short cone length [7], positive surgical margin status [256], and size of lesion [67] have been reported to be associated with an increased risk of persistent/recurrent disease [234567]. Two meta-analyses revealed that positive cone margin was a strong predictive factor of residual or recurrent disease [89]. Recently, the risk of obstetrical complication including preterm delivery, rupture of membrane, and low birth weight after conization, especially at depth >10 mm has been noted [101112]. Sufficient conization should be performed to avoid positive cone margin and obstetrical complication. In practice, we design conization according to colposcopic findings such as type of transformation zone (TZ) [1314] and position of the lesion. Several studies reported on appropriate cone depth [1516], but we found only one small study which reported appropriate cone length to avoid positive cone margin. This study examined the risk factors of positive cone margin and identified the appropriate cone length necessary to avoid positive cone margin.
MATERIALS AND METHODS
1. Study population
Patients who underwent conization with a diagnosis of CIN 2 or 3 at Kurume University Hospital between January 1999 and December 2010 were retrospectively studied. This study was approved by an Institutional Review Board of Kurume University. No patients with glandular lesion were included in this study.
2. Methods of conization and specimen processing
The cervix was exposed using a speculum under spinal anesthesia. Stay sutures of 1-0 Vicryl were positioned at the 3 and 9 o'clock position to occlude the descending branch of the uterine artery and to stabilize the cervix. After delineating the area of abnormality with 10% acetic acid, epinephrine diluted 1:100,000 with saline was injected at the 3, 6, 9, and 12 o'clock positions of the cervix with a 28 gauge needle. All specimens were marked for orientation with a suture at the 12 o'clock position. Conization was performed with a fine needle electrode, with a diathermy apparatus set to 40 watt (W) for cutting, and 40 W for coagulation. The base of the wound was cauterized with ball diathermy after excision. After the excisional procedure, endocervical curettage (ECC) was performed with a Kevorkian curette. The cone specimen was fixed with 10% formalin and processed with 12 serial sections per block. Preoperative cervical cytology was obtained by cytobrush and processed by conventional methods within 3 months of conization.
3. Management after conization
Patients who had positive cone margin and no wish for future pregnancy underwent subsequent hysterectomy by patient's choice. Patients who did not undergo subsequent hysterectomy were followed up every 3 months during the first year, every 6 months during the second year, and yearly thereafter. Patients underwent reconization or hysterectomy when high grade CIN was detected during follow-up.
4. Definitions and statistical analysis
Positive cone margin was defined as histological confirmation of CIN on the surgical margins as shown in Fig. 1 or in the specimens of ECC. Clinical factors, such as age, parity, preoperative cytological diagnosis, extent of disease divided into quadrants by colposcopy, type of TZ, and cone length of the conization specimen were selected as predictive factors. Each factor was compared with the incidence of positive cone margin. Size of disease was evaluated by abnormal colposcopic findings with number of cervical quadrants [13]. Not only ectocervical lesion but endocervical lesion which was visible by colposcopy was also taken into consideration for the evaluation of size of disease. Cone length was defined as the length between the ectocervical surface margin and the endocervical surface margin according to the International Federation for Cervical Pathology and Colposcopy (IFCPC) in 2011 (Fig. 1) [13]. Classification of TZ types was categorized as type 1, 2, or 3 according to site and visibility [1314].
Fig. 1
Definition of cone length. Cone length was defined as the length between ectocervical surface margin and the endocervical surface margin as defined by the International Federation for Cervical Pathology and Colposcopy in 2011.

The correlation between positive cone margin and each clinicopathological variables was tested by chi-square test, Fisher exact test or Student t-test. Univariable and multivariable logistic regression analyses were used to test for the value of other clinical and pathologic parameters in predicting positive cone margin. Cut-off value of cone length was estimated by logistic regression analysis with variables which were selected by stepwise methods. Hosmer-Lemeshow test was used to verify the fitness to the logistic model. Cut-off value of cone length was defined as length corresponds to estimated probability of positive cone margin equal to 0.1. We used the JMP ver. 11 (SAS Institute Inc., Cary, NC, USA) for statistical analyses. A p<0.05 was regarded as statistically significant.
RESULTS
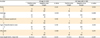
During the study period, 300 women who received conization with CIN 2/3 were enrolled. Patient characteristics were summarized in Table 1. Among 300 patients, 11 had CIN 2, and 289 had CIN 3. Positive cone margin was observed in 75 cases (positive endocervical margin, 68; ECC positive, 19). The mean age of the patients was 41.3±10.7 years old. The parity was 0 in 53 patients; the remaining 247 had a parity of 1 or more. Preoperative cytology was negative for intraepithelial lesion or malignancy in three cases, atypical squamous cell of undetermined significance in four cases, low-grade squamous intraepithelial lesion in 28 cases, high-grade squamous intraepithelial lesion in 225 cases, and squamous cell carcinoma (SCC) in 40 cases. Two or more quadrant disease was identified in 248 cases. TZ type 3 was observed in 15 cases. Positive endocervical margin was observed in 68 cases. The mean cone length was 17.8±4.5 mm. Table 2 lists clinicopathological factors in relation to positive cone margin. Preoperative cytology of SCC (p=0.006) and shorter cone length (p<0.001) had significantly higher rate of positive cone margin in total subjects. On the other hand, only shorter cone length (p<0.001) correlated with positive cone margin in women less than 40 years old.
Table 1
Patients' characteristics
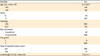
Table 2
Correlation between clinicopathological factors and cone margin status
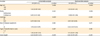
Univariable logistic regression analysis revealed that cytology of SCC (odds ratio [OR], 2.574; 95% CI, 1.275 to 5.126; p=0.007), and cone length (OR, 0.025; 95% CI, 0.004 to 0.136; p<0.001) were risk factors of positive cone margin. Multivariable logistic regression analysis revealed that cytology of SCC (OR, 4.014; 95% CI, 1.814 to 8.985; p<0.001), 2 or more quadrant disease (OR, 3.417; 95% CI, 1.304 to 10.312; p=0.011), and cone length (OR, 0.847; 95% CI, 0.785 to 0.911; p<0.001) were independent risk factors of positive cone margin (Table 3).
Table 3
Predictive factors for positive cone margin by univariable and multivariable analysis
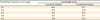
Next, we analyzed the cut-off value of cone length which was the most dominant risk factor of positive cone margin in women younger than 40 years old. In this group, cone length and size of disease were selected by stepwise methods. The estimated linear function by logistic regression analysis was as follows: y=2.837–0.295 (cone length)+0.791 (2 or more quadrant disease). Table 4 showed estimated cone length with the probability of positive cone margin among 0.1 and 0.5. Cone length for 10% of probability of positive cone margin was estimated as 15 mm in single quadrant disease and 20 mm in 2 or more quadrant disease, respectively.
DISCUSSION
In this study, we identified that preoperative cytology of SCC, 2 or more quadrant disease, and shorter cone length were independent risk factors of positive cone margin. Especially, shorter cone length was the most dominant risk factor of positive cone margin.
The definition of cone length has differed among various studies so far. In 2011, the IFCPC reported the definition of cone length as the distance from the distal or external margin to the proximal or internal margin of the excised specimen [13]. We found several studies which analyzed optimal cone length to avoid positive cone margin, but most of them analyzed cone depth rather than cone length [1516]. Milinovic et al. [17] reported the appropriate length of conizaiton as 18 mm in multiparous and 15 mm in nulliparous patients to secure a negative margin status, and that was the only study which analyzed appropriate cone length for CIN. In this study, we referred to the appropriate cone cut-off value in women younger than 40 years and identified the appropriate cone length as 15 mm in single quadrant disease and 20 mm in 2 or more quadrant disease with 0.1 of probability of positive cone margin. This value should be reasonable comparing from 23.0% of positive cone margin rate in women younger than 40 years of age. Because cervical length is one of the most important factors to maintain the pregnancy, we should try to minimize the cone length with obtaining the negative margin. Jakobsson et al. [18] reported that the risk for preterm birth was 2.45-fold higher when comparing large size or repeat conization with small or medium size conization. However, it is difficult to measure cone length during the procedure of conization. Ectocervical cutting point is decided by the location of TZ and disease. Therefore, cone depth will be the determinant of cone length.
We also showed that 2 or more quadrant disease and cytology of SCC as the risk factors of positive cone margin. Milinovic et al. [17] reported that more endocervical lesion was observed in cases of wide lesion. It might indicate the reason why 2 or more quadrant disease was a risk factor of positive cone margin in this study. To the best of our knowledge, this is the first report that preoperative cytology of SCC as a risk factor of positive cone margin. The incidence of SCC as preoperative cytology also correlated with 2 or more quadrant disease (p=0.007). On the other hand, it did not observe in women younger than 40 years old. It might be due to the small number of preoperative cytology of SCC in women younger than 40 years old.
In this study, we could not refer to the obstetrical outcome because the number of pregnancies after conization was small. Several studies reported on appropriate cone depth [1516], but we could not investigate it because of the lack of data. It would be interesting if we could compare cone depth and cone length.
In conclusion, we reported that shorter cone length, 2 or more quadrant disease and preoperative cytology of SCC were the risk factors of positive cone margin. We also identified optimal cone length according to the size of disease in women younger than 40 years old. Conization should be designed not only by colposcopic findings including type of TZ and size of disease, but also by cone length.
 XML Download
XML Download