

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In Korea, the incidence of ovarian cancer has been increasing gradually and was estimated to comprise 1.7% (2,374) of all newly diagnosed female cancers during 2015 [12]. Among gynecologic malignancies, ovarian cancer has the poorest survival rate owing to a lack of initial symptoms and effective screening tools, which results in relatively more advanced stage at diagnosis, and higher recurrence rates after treatment [1]. Moreover, it exhibits significant histologic heterogeneity and a wide variety of histologic features. The majority of ovarian cancers are epithelial ovarian cancers (EOCs; 90%) that are further grouped into different histologic subtypes [3].
Histologic subtype is a well-established prognostic factor in EOC [456]. Unlike serous carcinomas, most endometrioid carcinomas are identified at an early stage and tend to be relatively chemo-sensitive, consequently contributing to a better prognosis compared with other subtypes [789]. Clear cell carcinoma also presents at an early stage and has a relatively good prognosis. However, advanced stage clear cell carcinoma of ovary has a worse prognosis compared with serous or endometrioid carcinomas because it is less sensitive to platinum-based chemotherapy [1011]. Both endometrioid and clear cell carcinomas are associated with endometriosis, which is a common benign disease in women of reproductive age. Endometriosis is a known precursor of endometrioid and clear cell carcinomas, although the molecular mechanisms underlying the malignant transformation have not been elucidated fully [1213].
Although the prognosis and underlying carcinogenesis for EOC histologic subtypes are different, the current management strategies are the same. Extensive cytoreductive surgery and platinum-based adjuvant chemotherapy are commonly recommended for maximal survival [14151617]. Consideration of histologic subtypes is necessary to devise individualized treatment plans for patients with EOC. Knowing the exact distribution of each histologic subtype would be the initial step in facilitating such treatment plans; however, to our knowledge, the distribution in Korean women has not yet been evaluated.
Thus, this study aimed to investigate trends in the incidence of EOC, according to histologic subtypes, in Korean women between 1999 and 2012. This nation-wide database analysis was conducted through exploration of the Korea Central Cancer Registry (KCCR).
MATERIALS AND METHODS
1. Study design
This study was conducted as a subgroup analysis of the previously published study which reported nationwide cancer statistics in Korea [2]. In that study, incidence data between 1999 and 2012 had been obtained from the KCCR. For the current study, the data of primary EOCs and each histologic subtype during the same period were extracted and analyzed. Age-standardized incidence rates (ASRs) and annual percentage changes (APCs) in incidence rates were calculated. Patient data were divided into three groups based on age (<40, 40 to 59, and >59 years), and age-specific incidence rates were compared.
2. The Korea Central Cancer Registry
Historically, the KCCR began as a nation-wide, hospital-based cancer registry, set up by the Ministry of Health and Welfare in 1980. In 1999, the registry was expanded to cover the entire population [18]. Accurate nation-wide cancer incidence data is provided by the KCCR, named as the Korea National Cancer Incidence Database.
3. Classification of histologic subtypes
Based on the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3), data from women diagnosed with primary cancer of the ovary (C56) were retrieved. And those were converted according to the International Classification of Disease, 10th revision (ICD-10) [19]. Among them, only the data from those with EOCs including serous carcinoma, mucinous carcinoma, endometrioid carcinoma, clear cell carcinoma, adenocarcinoma not otherwise specified, other specified carcinoma, and unspecified carcinoma were analyzed. Non-EOCs such as sex-cord stromal tumors and germ cell tumors were excluded. Mixed cell adenocarcinomas consisting of different histologic subtypes were also excluded.
4. Statistical analyses
The ASRs were calculated using Segi’s world standard population [20]. For the estimation of trends in incidence rates for all EOCs and individual histologic subtypes, APCs were calculated as follows: [exp(β)-1]×100, and the regression coefficient (β) was obtained by a linear regression of log-transformed ASRs in a calendar year. Testing the hypothesis that the APC is equal to zero is equivalent to the hypothesis that the slope of the line in the equation is equal to zero. Statistical analyses were performed to test the trend. SAS 9.3 statistical software (SAS Institute Inc., Cary, NC, USA) was used for all calculations and a p<0.05 was considered statistically significant.
RESULTS
Overall, the number of newly diagnosed EOC cases between 1999 and 2012 has increased continuously: annual EOC cases increased from 922 in 1999 to 1,775 in 2012 (Table 1).
Table 1
Age-standardized incidence rates per 100,000 and annual percent changes (%) of epithelial ovarian cancer
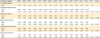
The ASRs and APCs for all EOCs and histologic subtypes are presented in Table 1, Fig. 1. The ASR for all EOCs has increased between 1999 and 2012, producing a significant APC over this period (2.53%; p<0.001). In 2012, the four most common histologic subtypes were serous, mucinous, endometrioid, and clear cell carcinoma.
Fig. 1
Age-standardized incidence rates (ASRs) per 100,000 of epithelial ovarian cancer in Korea between 1999 and 2012.

Among the four major histologic subtypes, the incidence of mucinous carcinoma alone decreased between 1999 and 2012, although the APC was not significant (–1.05%; p=0.131). By contrast, the incidences of serous carcinoma (APC, 4.34%; p<0.001) and endometrioid carcinoma (APC, 1.48%; p=0.032) increased significantly. During the same period, the incidence of clear cell carcinoma increased the most with statistical significance (APC; 8.13%, p<0.001).
Table 2, Fig. 2 show the ASRs and APCs for all EOCs and the four major histologic subtypes stratified according to age. Between 1999 and 2012, the incidence of EOCs increased significantly across all three age groups; the APCs were 1.87% for the younger age group (<40 years; p=0.001), 2.48% for the middle age group (40 to 59 years; p<0.001), and 3.02% for the older age group (>59 years; p<0.001). A trend of increasing APCs was observed as age increased. Similar findings were noted in serous carcinoma type.
Table 2
Age-specific incidence rates per 100,000 and annual percent changes (%) of epithelial ovarian cancer

Fig. 2
Annual percent changes (APCs, %) of epithelial ovarian cancer according to age groups between 1999 and 2012.

In mucinous carcinoma, the ASRs did not change significantly for the younger and middle age groups, whereas for the older age group, the incidence of mucinous carcinoma decreased with a significant APC (–2.74%; p=0.010). In endometrioid carcinoma, the ASRs increased within the younger age group with a significant APC (3.14%; p=0.007).
In clear cell carcinoma, the ASRs increased significantly across all age groups; the APCs were 10.00% for the younger age group (p=0.001), 7.39% for the middle age group (p<0.001), and 13.08% for the older age group (p=0.007).
The age-specific incidence rates for all EOCs and the four major histologic subtypes in 2012 are shown in Fig. 3. While the incidence of serous carcinoma was highest among patients in their early 60s, that of endometrioid carcinoma reached its peak among patients in their late 40s. The incidence of clear cell carcinoma was highest among patients with late 50s, and decreased thereafter.

DISCUSSION
In this study, a gradual increase in the incidences of EOCs was observed between 1999 and 2012. In Korea, the age-adjusted incidence rate of ovarian cancer is known to be much lower than that in Western countries. However, recent studies have reported that the incidence of ovarian cancers has been increasing continuously in Korea, and that this trend might be explained by the westernization of diet and life styles, as well as changes in sociodemographic factors [121]. Of the whole ovarian cancers, EOC is the most commonly identified (90%), and it is known to be affected by reproductive factors [3].
In 2012, the most common EOC histologic subtypes in Korean women were serous, mucinous, endometrioid, and clear cell carcinomas, representing 49.5%, 13.9%, 10.4%, and 10.3% of all EOC cases, respectively. Among the four major subtypes, we found statistically significant annual increases in serous, endometrioid, and clear cell carcinomas between 1999 and 2012. A similar trend was also observed in the study of another East Asian country, Taiwan [22].
However, in the current study, the incidence rate of mucinous carcinoma alone decreased between 1999 and 2012. There are a number of possible reasons for this decrease. First, recent advances have been made in the pathological diagnosis of ovarian mucinous carcinoma [23], suggesting that, before these advances, misdiagnoses of mucinous carcinoma could have led to overestimated incidence rates. For the precise distinctions between primary and metastatic ovarian mucinous carcinomas, pathologists began to utilize refined immunohistochemistry techniques. Prior to this, a substantial proportion of metastatic cases could have been misinterpreted as primary ovarian mucinous carcinomas [2425]. In addition, exclusion of borderline ovarian tumors, as well as pseudomyxoma peritonei, resulted in less common pure ovarian mucinous carcinoma cases than previously reported [26].
Second, influence of the reproductive factors on the development of EOCs might differ by histologic subtypes. Conditions suppressing ovulation, such as parity and oral contraceptive use, are known to have protective effects against EOC, more so for non-mucinous carcinomas compared with mucinous carcinomas [27282930]. In a case-control study, Soegaard et al. [29] reported that use of oral contraceptives was associated with a decreased risk of serous and endometrioid carcinomas, but not for mucinous carcinoma. Similarly, a meta-analysis of 45 epidemiological studies also concluded that the incidence of mucinous carcinoma was little affected by oral contraceptive use, whereas its protective effects against other subtypes were observed [30]. However, in Korean women, both the parity (total fertility rates per woman, 1.3 in 2013) and the prevalence of oral contraceptive use (percentage of women among those of reproductive age who are married or in union, 2.0% in 2009) are much lower than those in women from Western countries [3132]. Thus, combined protective effects of parity and oral contraceptive use might be reduced in Korean women, resulting in a relative increase in non-mucinous carcinomas.
Third, according to cohort studies and meta-analysis, cigarette smoking is related with an increased risk of ovarian mucinous carcinoma, but is not associated with an increased risk of serous or endometrioid carcinomas [3334]. Korea has the lowest prevalence for female cigarette smoking among the Organization for Economic Co-operation and Development member countries (5.8% in 2012) [35], which might explain the relatively low incidence rate of mucinous carcinoma.
In this study, the incidence rate of clear cell carcinoma between 1999 and 2012 increased markedly across all age ranges, which was consistent with the results of a study in Taiwanese women [22]. Interestingly, whereas clear cell carcinoma constitutes only a small portion of EOCs in Western country, it accounts for approximately 20% of EOCs in Japan, another East Asian country [36].
Causes for the marked increase in the clear cell carcinoma type in Korean women might be explained by endometriosis, a common gynecologic disorder that occurs in 5% to 10% of reproductive-age women. Women with endometriosis are predisposed to developing EOC, with the risk of clear cell carcinoma being 3-fold greater than that of the other histologic subtypes [121337]. In addition, endometriosis is associated with excessive estrogen exposure [38]. For the Korean women, westernization of diet and life styles has led to earlier menarche, increased obesity, and decreased childbearing [2139]. All these conditions are associated with an increased exposure to estrogen and might influence the prevalence of endometriosis, resulting in a consequential increase in ovarian clear cell carcinoma.
As mentioned earlier, histologic subtype is a prognostic factor for the patients with EOC [456]. Although stage at diagnosis, sensitiveness to platinum-based chemotherapy, recurrence after treatment, and survival is known to be different among the types [78910111213], the current management strategies are the same [14151617]. However, efforts to devise specific treatments according to histologic subtypes of EOC have been made. A Japanese randomized controlled trial in patients with ovarian clear cell carcinoma (JGOG3017/GCIG) is the representative. In this trial, the efficacy of an irinotecan-cisplatin regimen was compared with a conventional paclitaxel-carboplatin regimen as a first line chemotherapy. Although the irinotecan-cisplatin regimen did not show a survival benefit, it was suggested as an alternative treatment choice for ovarian clear cell carcinoma because of the different toxicity profile [40]. Like this trial, further studies, which explore individualized treatment strategies for specific EOC histologic subtypes, are encouraged indeed.
Up to our knowledge, the current study is the first to report the incidence rates of EOC according to histologic subtypes in Korea. Nevertheless, this study has several limitations. Patients' demographic characteristics, except age at diagnosis, were not obtained. Detailed information including cancer stage, treatment courses, and survival data were also not investigated. Whether the changes in pathological diagnostic criteria were reflected in the database was not clear. In addition, recent simplified classification systems that assign EOC into type I and type II, according to morphological, molecular, and clinical features, have not yet been employed in the database. Despite these limitations, secular trends in incidence rates of all EOCs and individual histologic subtypes were clearly demonstrated.
In conclusion, the incidence of EOC increased continuously from 1999 to 2012 in Korea. Among the four major histologic subtypes, only the incidence of mucinous carcinoma has decreased; however, without significance. During the same period, ovarian clear cell carcinoma has remarkably increased in all ages. Identification of precursors and carcinogenesis courses for each histologic type are needed to understand its nature. By the efforts to reveal proper treatment methods and their impact on survival, more individualized treatment plans could be provided for the patients.
 XML Download
XML Download