

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Based on epidemiological and laboratory studies, human papillomavirus (HPV) is considered a primary cause of uterine cervical cancers. The global prevalence (in 22 countries) of HPV in cervical cancers is 99.7%; therefore, virtually all cervical cancers have HPV infection [1]. After the initial HPV infection, squamous cell carcinoma (SCC) of the cervix develops through a lengthy stage of squamous intraepithelial lesion (SIL), which is a precursor lesion. However, most HPV infections are transitory, and only a small fraction of infections persist and progress to high-grade squamous intraepithelial lesion (HSIL) and invasive cancer, which suggests that other co-factors contribute to cancer occurrence after HPV infection. To reduce the incidence of cervical SCC, it is important not only to diagnose and treat SIL through cytological screening but also to discover and remove co-factors that are involved in HPV persistence and development into SIL and SCC.
Certain HPV types and HPV viral load are considered factors associated with the persistence of HPV infection and progression to cancer [23]. In addition, there are a few associated environmental factors including high parity [4], long-term use of oral contraceptives [5], smoking [6], human immunodeficiency virus (HIV) infection [7], and sexually transmitted infections (STIs) other than HPV and HIV [8]. In particular, STIs not only play a role as a co-factor in the onset of cervical cancer but are also causative diseases with serious long-term sequelae such as chronic pelvic inflammatory disease, infertility, and/or ectopic pregnancy; therefore, accurate diagnosis and treatment are important [9].
There have been several studies regarding the role of STIs in the development of SIL and invasive cervical cancer in HPV-infected women. Chlamydia trachomatis (C. trachomatis) is the most frequently investigated and has a demonstrated association with HPV infection, especially high-risk HPV, SIL, and invasive SCC [1011121314]. However, there was no association with glandular lesions including in situ adenocarcinoma, invasive adenocarcinoma, or adenosquamous carcinoma; therefore, the role of C. trachomatis in cervical carcinogenesis might be restricted to squamous cell malignancy [1015]. According to a pooled analysis of seven case-control studies of invasive cervical cancer by the International Agency for Research on Cancer, herpes simplex virus infection might act in conjunction with HPV infection to increase the risk of invasive cervical carcinoma including both squamous and adenocarcinomas [16]. In addition, Trichomonas vaginalis (T. vaginalis), Mycoplasma, and Ureaplasma species have been associated with HPV infection and abnormal cervical cytology [17181920].
In the present study, HPV DNA and STI tests were performed for Obstetrics and Gynecology outpatients who showed abnormal cervical cytology to investigate the correlations between STIs with high-risk HPV and abnormal cervical cytology and to examine the meaning and usefulness of STI tests when caring for patients with abnormal cervical cytology and/or positive results on a high-risk HPV DNA test.
MATERIALS AND METHODS
1. Study population
The study population consisted of women who had undergone a cervical cytology test using a liquid-based cytology technique and an HPV DNA test at the Obstetrics and Gynecology outpatient clinic at Cheil General Hospital & Women's Healthcare Center Clinic between January 2012 and May 2013. The remaining DNA from the DNA extracted from the liquid-based cytology specimen of the cervix used for the HPV DNA test was used in the STI test. Cervical cytology samples were collected and prepared using a liquid based cytology technique (SurePath, TriPath Imaging Inc., Burlington, NC, USA) according to the manufacturer's protocol and were diagnosed following a routine schedule without prior information on the HPV DNA test results. Cytological diagnoses were determined using the 2001 Bethesda system, from which 200 cases of atypical squamous cells of undetermined significance (ASC-US), 200 cases of atypical squamous cells-cannot exclude high grade squamous intraepithelial lesion (ASC-H), 200 cases of low-grade squamous intraepithelial lesion (LSIL), and 200 cases of HSIL were selected. For the control group, 200 cases of negative cervical cytology results (negative for intraepithelial lesion or malignancy [NILM]) were selected, resulting in a total of 1,000 cases for analysis. The study was approved by the Institutional Review Board of Cheil General Hospital & Women's Healthcare Center, and all participants provided informed consent.
2. DNA extraction
DNA was extracted from cervical cytology samples using an AccuPrep Genomic DNA Extraction kit (Bioneer Co., Daejeon, Korea) according to the manufacturer's protocol. In brief, cell pellet from 1.5 mL cervical cytology sample was washed in phosphate buffered saline (PBS) buffer and reacted at 60°C for 20 minutes in 200 µL PBS buffer mixed with 20 µL proteinase K. Then, 100 µL isopropanol was added and mixed well, followed by transfer to a binding column for centrifugation, which was performed with two washes with washing buffer. The binding column was transferred to a new tube, and elution buffer was added to elute the bound DNA, which was then centrifuged to finally obtain the DNA solution. The DNA solution was used in the HPV DNA test immediately after extraction, and the remaining DNA solution was stored at –20°C for the STI test.
3. HPV DNA test
The HPV DNA test was performed using a Seeplex HPV4A ACE Screening kit (Seegen Inc., Seoul, Korea) following the manufacturer's protocol; 4 µL of 5× HPV4A ACE PM (primer mixture including primer pairs for HPV, a primer pair for internal control, and template of internal control), 3 µL of 8-methoxypsoralen solution, and 10 µL of 2× Multiplex Master Mix (containing DNA polymerase and buffer with deoxyribonucleotide-5'-triphosphate [dNTP] and dye) were mixed to form 17 µL of polymerase chain reaction (PCR) master mix, to which 3 µL of DNA solution extracted from the specimen was added to prepare a mixture with a total volume of 20 µL for the PCR reaction. Positive and negative controls were used from the kit. The PCR reaction was performed using a GeneAmp 9700 PCR System (Applied Biosystems, Carlsbad, CA, USA). After a pre-heating step at 94°C for 15 minutes, 40 amplification cycles were performed, with denaturation at 94°C for 30 seconds, annealing at 60°C for 90 seconds, and extension at 72°C for 90 seconds. Amplification was completed with a final extension step at 72°C for 10 minutes. A MultiNA Microchip Electrophoresis System (Shimadzu, Tokyo, Japan) was used for detection of amplified products. The Seeplex HPV4A ACE Screening kit is capable of isolating HPV types 16 and 18, as well as detecting 16 high-risk types (High-Risk HPV Common, HRC, types 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82) and the low-risk HPV types 6 and 11, using a multiplex PCR method. The HPV DNA test results were divided into two groups: high-risk HPV positive group (positive for any of HRC or HPV types 16 and 18) and high-risk HPV negative group (negative for HRC and HPV types 16 and 18) regardless of HPV type 6 and 11 positivity.
4. STI test
The causative micro-organisms for STIs were examined with the remaining DNA using an Anyple II STI-7 Detection kit (Seegen Inc.) according to the manufacturer's protocol. This kit is newly designed to simultaneously detect seven types of causative microorganisms for STIs (C. trachomatis, Neisseria gonorrhea, Mycoplasma genitalicum (M. genitalicum), Mycoplasma hominis, Ureaplasma urealyticum, Ureaplasma parvum (U. parvum), and T. vaginalis) using real-time PCR, which offers more accurate results than other STI test methods [21]. A mixture of 5 µL 4× STI-7 TOM (TOCE Oligo Mix), 5 µL 4× Anyplex PCR Master Mix (with uracil-DNA glycosylase [UDG], containing DNA polymerase, UDG, and buffer with dNTPs), and 5 µL RNase-free water was prepared as the 15 µL PCR master mix, to which 5 µL of DNA solution extracted from the specimen for testing was added for a total of 20 µL for use in the PCR reaction. For the positive and negative controls, the positive control and RNase-free water from the kit were used instead of the DNA extracted from the specimen. The real-time PCR reaction was performed using the CFX96TM Real-Time PCR Detection System (Bio-Rad Laboratories, Hercules, CA, USA). After an initial incubation at 50°C for 4 minutes and pre-denaturation at 95°C for 15 minutes, 50 cycles of alternating incubations (95°C for 30 seconds, 60°C for 1 minute, and 72°C for 30 seconds) were performed. The melting temperature was analyzed by increasing the reaction temperature from 55°C to 85°C (0.5°C/5 seconds).
5. Statistical analysis
Statistical analysis was performed using SAS ver. 9.3 (SAS Institute Inc., Cary, NC, USA). Data are reported as numbers (percentages) or odds ratios (ORs) with the corresponding 95% CIs. The associations between STIs and high-risk HPV infection were determined using logistic regression analysis. To compare the STI positive rates based on cytological diagnosis and age of patients, chi-square tests or Fisher exact tests were performed. A p<0.05 was considered significant.
RESULTS
1. Correlations between STIs and high-risk HPV
Despite the significant correlation between total STIs and high-risk HPV (p=0.0057), there was no significant correlation between each microorganism and high-risk HPV in Table 1. The probability of testing positive for high-risk HPV was 1.47 times higher with total STIs (+) than total STIs (−) (OR, 1.47; 95% CI, 1.12 to 1.93; p=0.0058). The probabilities of high-risk HPV (+) were 2.07 and 2.23 times higher when C. trachomatis and M. genitalicum were positive than when negative, respectively; these were not statistically significant.
Table 1
Correlations between STIs and HR-HPV infection
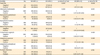
Values are presented as number (%).
HR-HPV, high-risk human papillomavirus; OR, odds ratio; STI, sexually transmitted infection.
*Negative for all micro-organisms of STI. †Positive for any microorganism of STI including multiple infections.
![]()
2. Correlations between high-risk HPV and STIs with abnormal cervical cytology
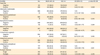
As expected, as abnormal cervical cytology became more severe, the positive rate for high-risk HPV significantly increased (p<0.0001) in Table 2. The positive rates for total STIs, M. genitalicum, and multiple infections (>1 organism) were significantly different according to the cervical cytology results (p=0.0181, p=0.0219, and p=0.0136, respectively) in Table 2. The positive rate for total STIs was significantly higher in all of the groups with abnormal cervical cytology except ASC-US than in the normal (NILM) group, and the positive rates for M. genitalicum were significantly higher in the LSIL and HSIL groups than in the ASC-US group in Table 3. For multiple infections, the LSIL group showed a significantly higher positive rate than the other cytological diagnosis groups.
Table 2
Correlations between HR-HPV and STIs with abnormal cervical cytology
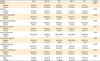
Values are presented as number (%).
ASC-H, atypical squamous cells, cannot exclude high grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; HR-HPV, high-risk human papillomavirus; HSIL, high-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; LSIL, low-grade squamous intraepithelial lesion; STI, sexually transmitted infection. *Negative for all micro-organisms of STI. †Positive for any microorganism of STI including multiple infections.
![]()
Table 3
Correlations between STIs and abnormal cervical cytology (pairwise comparison)

ASC-H, atypical squamous cells, cannot exclude high grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; STI, sexually transmitted infection.
*Compared to NILM group. †Compared to ASC-US group.
![]()
3. Correlations between STIs and ASC-H+
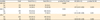
The probability of grades equal to or higher than ASC-H results from the cervical cytology was significantly higher in patients testing positive for total STIs (1.46 times), C. trachomatis (3.21 times), or M. genitalicum (3.58 times) than in those testing negative in Table 4.
Table 4
Correlations between STIs and cytological diagnosis of ASC-H+
Values are presented as number (%).
ASC-H, atypical squamous cells, cannot exclude high grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesion or malignancy; OR, odds ratio; STI, sexually transmitted infection.
*ASC-H+LSIL+high-grade squamous intraepithelial lesion.
![]()
4. Correlations between STIs and abnormal cervical cytology according to high-risk HPV results
In the high-risk HPV (+) group, there were no significant differences in STIs based on abnormal cervical cytology. In the high-risk HPV (−) group, a significantly higher total STIs positive rate was present in the group with grades equal to or higher than ASC-US results from the cervical cytology than the group with normal results (OR, 1.87; 95% CI, 1.20 to 2.90; p=0.0053) in Table 5. However, there were no differences in the total STIs positive rates between the groups with or without grades equal to or higher than ASC-H results from the cervical cytology or the groups with or without grades equal to or higher than LSIL results from the cervical cytology.
Table 5
Correlations between abnormal cervical cytology and STIs in HR-HPV (–) cases
Values are presented as number (%).
ASC-H, atypical squamous cells, cannot exclude high grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; HR-HPV, high-risk human papillomavirus; LSIL, low-grade squamous intraepithelial lesion; OR, odds ratio; STI, sexually transmitted infection.
*ASC-US+ASC-H+LSIL+high-grade squamous intraepithelial lesion (HSIL). †ASC-H+LSIL+HSIL. ‡LSIL+HSIL.
![]()
5. STIs and age
Significantly higher positive rates for total STIs, C. trachomatis, and M. genitalicum were present in those aged <50 years than in those aged ≥50 years in Table 6.
Table 6
Prevalence of STIs according to age groups

![]()
DISCUSSION
In the present study, STI tests were performed with samples from 800 cases of abnormal cytology of squamous cell origin to investigate the correlations with high-risk HPV and cytological diagnosis and examine the effects on diagnosis and treatment. As a result, there was a significant association between total STIs and high-risk HPV infections, in which STI (+) cases had a 1.47 times higher positive rate for high-risk HPV than STI (−) cases, regardless of the type of causative microorganism. A number of previous studies showed that specific STI-causative micro-orgamisms (C. trachomatis, herpes simplex virus-2, Mycoplasma species, Ureaplasma species, and T. vaginalis) were correlated with HPV infection, SIL, and cervical cancer risk, although a few studies reported that C. trachomatis and herpes simplex virus-2 had no associations with HPV, abnormal cytology, SIL, or cervical cancer risk [22232425]. The probabilities of testing positive for high-risk HPV in patients who were C. trachomatis (+) and M. genitalicum (+) were 2.07 and 2.23 times higher, respectively, but these were not statistically significant. Consequently, correlations between specific STI causative microorganisms and HPV could not be found in the present study.
However, as expected, there was a strong correlation between abnormal cervical cytology and high-risk HPV infection, while STIs were correlated with abnormal cervical cytology. The rates of total STIs, M. genitalicum, and multiple concurrent STIs were significantly different according to cytological diagnosis, of which the total STIs positive rate was significantly higher in all of the abnormal cytological diagnosis groups, except the ASC-US group, when compared with the normal group. Regarding M. genitalicum, a significantly higher positive rate was observed in the SIL group than in the ASC-US group, while the positive rate of multiple concurrent STIs was higher specifically in the LSIL group than in the other groups. In addition, when the cervical cytology results were divided into groups based on severity for comparisons, the probabilities of having a cytological diagnosis of grades equal to or higher than ASC-H were significantly higher in patients who tested positive for total STIs, C. trachomatis, or M. genitalicum than in patients who tested negative by factors of 1.46, 3.21, and 3.58 times, respectively. Previous studies have also shown that the rates of specific STI-causative microorganisms are significantly correlated with the severity of abnormal cervical cytology [11171926]. Thus, checking the cervical cytology results is important for STI (+) patients, particularly for C. trachomatis (+) or M. genitalicum (+) patients. Moreover, these results should encourage follow-up measures such as histologic diagnosis through tissue biopsy and appropriate treatment. In patients with a cytological diagnosis of grades equal to or higher than ASC-H, appropriate evaluation and treatment for STIs as well as SIL should be conducted.
The results also suggest that cytological changes diagnosed as ASC-US in women without high-risk HPV could be false positive due to inflammation and cytological changes of cervical epithelial cells induced by the STI. The previous studies showed that some STI-causative micro-orgamisms were able to change in the size and shape of cervical epithelial cells, and reproductive tract infections were the second most common cause of ASC-US overdiagnosis [272829]; women who were high-risk HPV (−) had higher total STIs positive rates with cytological diagnosis of grades equal to or higher than ASC-US than with normal cytology, while there were no differences with a cytological diagnosis of grades equal to or higher than ASC-H or than LSIL. The HPV DNA tests used in the present study did not detect the low-risk HPV types, except for HPV types 6 and 11, and the positive and negative groups were based on the presence or absence of the high-risk HPV types. Therefore, it is possible that patients infected with the low-risk HPV types could have been classified in the high-risk HPV (−) group. However, previous studies have demonstrated that the high-risk group accounted for 59% (63% for patients <30 years of age) among those with HPV detected with ASC-US [30], and 90% of HPV infection cases with ASC-US were high-risk HPV (+) [31]. Therefore, detecting only the high-risk HPV types is expected to include more than half of cases infected with HPV in the ASC-US group. As such, if a patient is high-risk HPV (−) and the cervical Pap smear results indicate ASC-US, it is valid to consider the possibility of cytological changes caused by STIs in addition to the low-risk HPV types. Moreover, since high-risk HPV persistence is more important than HPV infection itself for the onset of cervical cancer, the evaluation of STIs rather than infection with the low-risk HPV types should be more helpful for appropriate diagnosis and treatment.
Finally, the comparisons based on age (<50 years vs. ≥50 years) resulted in higher positive rates for total STIs, C. trachomatis, M. genitalicum, and (U. parvum) in the younger age group. Considering that STIs are related with sexual activities, this result is not surprising. Because STIs can cause severe sequelae, such as pelvic inflammatory disease or infertility, it is necessary to conduct more aggressive evaluations for STIs during outpatient clinic examinations for women of childbearing age. In particular, close attention should be given to pregnant women because STIs can increase perinatal morbidity and mortality, including preterm birth, low birth weight, and neonatal death [93233].
The present study demonstrated that there was a significant correlation between STIs and high-risk HPV infection and that the positive rates of total STIs, C. trachomatis, and M. genitalicum with a cervical cytology of grades equal to or higher than ASC-H were significantly higher than those who had less severe grades. Moreover, cytological diagnosis, especially of ASC-US, was influenced by STIs when the high-risk HPV types were negative. Therefore, performing high-risk HPV test and cervical cytology for patients who are STIs (+) should be helpful to determine the appropriate diagnosis and treatment. In addition, for patients who are diagnosed with grades equal to or higher than ASC-H based on cervical cytology should also undergo STI test as well as HPV DNA test to identify co-infections and administer appropriate treatment. For patients who are high-risk HPV (−) with cytologic diagnosis of ASC-US on a cervical smear, it is necessary to check for STIs while considering the chance of false positive results from the cytological diagnosis. Meanwhile, women of childbearing age had a higher positive rate for STIs than women of post-menopausal age. Therefore, owing to the adverse effects of STIs on fertility and the fetus, it is necessary to perform more aggressive STI evaluations for women of childbearing age, particularly pregnant women.
 XML Download
XML Download