

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine cancer is the most common form of gynecological cancer in the United States with 49,560 new cases and 8190 deaths estimated in 2013 [1]. Surgery is the mainstay for staging and optimizing treatment for women with endometrial carcinoma.
The surgical approach has rapidly evolved since the late 1980s with the introduction of laparoscopy in the surgical staging of endometrial cancer [2]. In 2005, the U.S. Food and Drug Administration cleared the da Vinci robotic computer based platform (Intuitive Surgical Inc., Sunnyvale, CA, USA) for gynecology, adding another tool to our armamentarium in the management of endometrial cancer.
An alternative to conventional laparoscopy or robotic surgery is the laparoendoscopic single-port surgery (LESS) [3], which further improves the cosmetic benefits of minimally invasive surgery while avoiding the potential morbidity associated with multiple incisions [4]. Although LESS is innovative, it presents some unique challenges, such as instrument crowding, loss of depth perception, and need for significant laparoscopic skills. In an attempt to solve the problems of single-incision techniques, recently, novel single-site instruments and accessories for the da Vinci Si System have been developed and tested in preliminary cadaveric and human studies [56]. Recently, our study group confirmed the potential benefits related to the robotic single-site approach [7].
The aim of this study was to compare robotic single-site hysterectomy (RSSH) versus robotic multiport hysterectomy (RMPH) in early stage endometrial cancer in terms of surgical outcomes and costs.
MATERIALS AND METHODS
This is a retrospective case-control study, comparing perioperative outcomes and costs of RSSH (cases) and RMPH (controls) in early stage endometrial cancer patients. RSSH were matched 1:2 to a number of patients selected from 130 patients who received RMPH at our institution between August 2010 and December 2011. In fact, in our institute early endometrial cancer was operated by robotic multiport system from August 2010 to December 2011 when we had access to the robotic single-site system. The criteria for matching were as follows: age, body mass index (BMI), comorbidity, the International Federation of Gynecology and Obstetric (FIGO) stage, type of radical surgery, histologic type, and grading.
1. Study design and data collection
Patients were operated on by the same surgeon (EV), and the same surgical team who have an optimal experience both by laparotomy and laparoscopic technique, using the da Vinci Si Surgical System at the Gynaecologic Oncologic Unit, "Regina Elena" National Cancer Institute, Rome, Italy.
The main inclusion criteria were a clinical diagnosis of early stage endometrial cancer (FIGO stage IA/IB), confirmed at the definitive histological examination, and a histologic diagnosis of endometrioid adenocarcinoma. We excluded patients with anesthesiological contraindications for minimally invasive approach (obese patients who could not sustain a steep Trendelenburg position) and patients with large uterine requiring morcellation. Prior abdominal surgery was not considered part of the exclusion criteria. Pre-treatment evaluation included: medical history collection, physical examination, vaginal-pelvic examination, chest X-ray, ultrasound scan, and pelvic magnetic resonance imaging scan. Approval to conduct the study was obtained independently from an Institutional Review Board (IRB) of Regina Elena National Cancer Institute. Informed consent to RSSH or RMPH was obtained from all patients in accordance with local and international legislation (Declaration of Helsinki) [8]. All the patients who underwent robotic surgery were informed that the procedure could have been converted to laparoscopy or laparotomy if necessary.
Clinical patient characteristics including age, BMI, and clinical stage according to the FIGO classification, tumor grade, comorbidity such as diabetes and/or hypertension and prior abdominal surgery were recorded. Intraoperative parameters including operative time, blood loss, conversion rate, and complications were recorded as well. Moreover, blood transfusions were performed if hemoglobin value was ≤7 g/dL. Operating time was defined from the beginning of skin incision to completion of skin closure. The estimated blood loss (EBL) was calculated by the difference in the total amounts of suctioned and irrigation fluids. Pelvic lymphadenectomy was performed based on frozen section analysis of the uterus (i.e., myometrial invasion >50%, and grade 2 or 3). Postoperative parameters included short term (within 30 days of the procedure), and long term complications (more than 30 days after the procedure), length of hospitalization, median follow-up duration, recurrence, and disease-free interval. Complications were defined according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 [9]. Moreover, status of the surgical margins, status, and number of removed pelvic lymph nodes and length of dissected vagina were evaluated.
Mean hospital cost per discharge was calculated summarizing the cost of daily hospital room charges, operating room (surgeon costs, anesthetist costs, pharmacy costs, anesthesia requirements, equipment used, and operative time), costs of supplies, and length of hospital stay. The cost of the operating room and hospital days were calculated by evaluating the mean operative time and hospital days for each group.
2. Surgical technique
All patients have antibiotic prophylaxis (Augmentin 2.2 g intravenously) and perioperative low molecular weight Enoxaparin (40 mg/day subcutaneously). The vaginal cavity is cleansed with povidone iodine solution and a Foley catheter is placed in the bladder. No uterus manipulator devices were used, but the cervix was closed with a modified tenaculum called “simple nebs arising incision landmark” (SNAIL) [10]. A medical grade silicone balloon, named colpo-pneumo occluder (Cooper Surgical, Trumbull, CT, USA) was also emplaced in the vagina in order to preserve an adequate pneumoperitoneum during colpotomy. In addition, intraoperative lower extremity sequential compression devices for venous thrombosis prophylaxis are used. All procedures were performed under general endotracheal anesthesia, a careful inspection of the entire abdominal cavity was performed with the robotic endoscope in order to identify any suspicious peritoneal lesion that would exclude the patient from having the procedure completed by robotic technique and peritoneal washing was routinely performed. In all patients, uterine, ovarian, and vaginal vessels were coagulated using the new bipolar Maryland in RSSH group and PK in RMPH group. Moreover, the uterus and the adnexa were extracted throughout the vagina, the vaginal vault was closed with single stitches using the vaginal way and each layer of the access port was sutured separately. In all cases the urine catheter is removed 12 hours after surgery and the criteria for discharge was a recovery of rectal and vesical function and absent of pain.
1) RSSH
A 2 cm long incision over the lower rim of the umbilicus, down to the level of the fascia was performed after lubrication of the Single-site port (Intuitive Surgical) by dipping in a sterile solution (e.g., saline or water). Using an atraumatic clamp, the Single-site port was grasped just above the lower rim. The leading edge of the folded port was inserted into the incision with a downward motion, while counter-traction was provided by retractors within the incision (Fig. 1A). Insufflation to reach a pneumoperitoneum of approximately 12 mm Hg was started. Then, the table was placed in the Trendelenburg position (30°). A da Vinci Si 8.5 mm 30° endoscope was inserted vertically and used during the whole course of surgery. After, a 5×250 mm curved cannula (Arm 2) was lubricated and inserted through the designated lumen while the external rim of the port was held by the assistant to avoid displacement. The cannula was guided near to the uterus and then held still to allow docking. This was done by holding the cannula still in one hand while the other hand brings and mounts the arm to the second 5×250 mm curved cannula (Arm 1). Finally, the instruments were introduced: a monopolar spatula on Arm 2 and a bipolar Maryland on Arm 1. The assistant's 5 mm accessory cannula, with which the assistant holds and moves either a suction/irrigator or a 5 mm endo-clip instrument, was inserted last of all. Class A plus bilateral salpingo-oophorectomy RSSH according to Querleu and Morrow classification [11] was performed.

2) RMPH
Patients were placed in the lithotomy position with the arms tucked at each side. After the creation of a pneumoperitoneum to 12 mm Hg with a transumbilical Veress needle, a 12-mm trocar was placed at 5 cm cranial to the umbilical level. Three 8-mm trocars, specific for the da Vinci robotic systems (Intuitive Surgical) were placed: one (Arm 1) on the right side of the abdominal wall, medial and cranial to the right anterior upper iliac spine, and two on the left side of the abdominal wall. The first (Arm 2) on the left lowest rib and the second (Arm 3) medial and cranial to the left anterior upper iliac spine on the same line of the right trocar, and fastened to the robotic arms. An assistant 10-mm trocar was placed on the right side of the abdominal wall, 7 to 10 cm laterally, from the supraumbilical trocar (Fig. 1B). After we obtained the Trendelenburg position (30 grade), the da Vinci robotic column was positioned near the operating table between the patient's feet and docked. The instruments were introduced: a bipolar grasper and a PK grasper on the left robotic trocars (Arms 2 and 3, respectively), and a monopolar scissor on the right robotic trocar (Arm 1). A 30 grade Surgical Intuitive endoscope was used during all operations. Class A plus bilateral salpingo-oophorectomy RMPH according to Querleu and Morrow classification [11] was performed.
3. Statistical analysis
Descriptive statistics were performed on characteristics of patients. The chi-square, Fisher exact, and Mann-Whitney U-tests were used when comparing categories against categorical and continuous data, respectively. A p<0.05 was considered statistically significant. SPSS ver. 21.0 (IBM Co., Armonk, NY, USA) was used for all statistical evaluations. The matching was performed using Propensity Score Matching methods, by using a nearest neighbor matching algorithm that pairs patients with the closest propensity scores within a defined limit (calipers of width equal to 0.2)
RESULTS
A total of 23 women who underwent RSSH between December 2011 and November 2013 were matched with 46 historic controls treated by RMPH in the same institution, with the same surgical team, between August 2010 and December 2011.
1. Patient's characteristics
No significant differences between groups were observed (Table 1). A large part of the RMPH group were prior submitted to abdominal surgery (72.5%) whereas only 43.5% of patients in RSSH group (p=0.021) with a different frequency of the presence of pelvic adhesion in RMPH (54.3%) and RSSH (30.4%) group (p<0.001). No significant difference were found in comorbidity rate between the two groups (p=0.561).
Table 1
Clinical characteristics
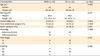
Values are presented as number (%).
BMI, body mass index; FIGO, The International Federation of Gynecology and Obstetric; IQR, interquartile range; RH, robotic hysterectomy; RSSH, robotic single-site hysterectomy.
![]()
2. Perioperative parameters
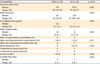
Patients in the RSSH group had about the same median operative time of the control group with 110 and 102.5 minutes, respectively (Table 2). The median EBL was 50 mL in the RSSH group and 100 mL in the RMPH, while the median drop of hemoglobin before and 24 hours after operation in the RSSH and RMPH was 0.6 g/dL (range, 0.1 to 1.5 g/dL) and 1 g/dL (range, 0.1 to 2.5 g/dL), respectively. These differences were statistically significant (p≤0.001). Neither in RSSH than in RMPH were intraoperative complications observed. No conversion to laparotomy or laparoscopy was necessary. Final pathologic findings were similar between the two groups in terms of FIGO stage and grading. The vaginal margin lengths and number of pelvic lymph nodes removed were similar in the two groups. In giacobix1 RMPH group, seven lymphadenectomies were performed in IB FIGO stage G3 endometrial cancer and six in IB FIGO stage G2 endometrial cancer. In RSSH group, a further two pelvic lymphadenectomies were performed in IB FIGO stage G3 endometrial cancer and two in IB G2 endometrial cancer. Definitive histologic results confirmed the frozen section examination: all of the specimens were diagnosed as endometrioid adenocarcinoma FIGO stage IA (71.7% in RMPH and 82.6% in RSSH group respectively) and FIGO stage IB (28.3% in RMPH and 17.4% in RSSH, respectively). The total amount of lymph nodes retrieved were negative for metastasis. The median length of hospital stay was 2 days in the RSSH group and 3 days in the RMPH group (p≤0.001).
Table 2
Surgical outcome
![]()
3. Postoperative parameters and further management
The incidence of early and late complications among groups was not statistically significant. After RSSH, one patient required laparoscopic re-intervention to control postoperative bleeding from the small vaginal artery while two patients in the RMPH group required blood transfusion. In the RMPH group, one patient had a high fever (grade 2 according to CTCAE v4.03) that required prolonged antibiotic therapy.
The median follow-up was 41.4 months (range, 27.2 to 50.1 months) for RSSH group and 56.4 months (range, 8 to 66.9 months) for RMPH group. Two (8.7%) and seven patients (15.2%) in RSSH and RMPH group respectively with high-risk disease (stage IB; G3) underwent further adjuvant radiotherapy. We didn't have recurrence in RSSH group while we had one relapse in RMPH group: a patient (stage IA; G3) had lung metastasis 12 months after robotic surgery. She underwent platinum based chemotherapy but died of disease 20 months after surgery.
4. Costs
The costs of the operating room were greater in the RSSH than in the RMPH group (Table 3). This difference was due to the increased operative time employed in the RSSH group. Length of hospital stay accounted for 20.9% of the variance in total cost in both of the two groups. Most of the whole budget spent for the procedure consisted of the costs of disposable robotic equipment, 58.2% of total costs for RMPH and 45.4% for RSSH. Medical management costs were not calculated but we underline that the number of specialized surgeons needed for the procedure were the same for both RMPH and RSSH.

DISCUSSION
Our retrospective study suggests the safety and feasibility of RSSH for staging early endometrial cancer without major differences from the RMPH in terms of surgical outcomes, but with lower hospital costs. The concept of LESS is based on the minimization of skin incision to gain access to the abdominal or pelvic cavities to perform surgical procedures. This concept might translate into a benefit for patients in terms of port-related complications, recovery time, pain, and cosmesis [1213]. This approach is to be considered as a safe and feasible technique; however, loss of triangulation, instrument crowding and clashes, poor visualization, and ergonomic problems are the most challenging issues surrounding the use of LESS [3].
The robot permits the surgeon to overcome some technical problems avoiding tremors, offering the 3 dimensional-vision and instruments that can be precisely moved in a complete 360°. Otherwise multiport robot technique produces optimal surgical results but leave the patients multiple scars. Fagotti et al. [14] stated that surgical scars should not be considered a “cosmetic problem” but a reflection of the impact body image has on the patient perpetually reminding them of the cancer. The single-site access (“scar free surgery”) truly provides the solution to this problem proposing a minimal incision through the umbilicus access alone (Fig. 2).
 | Fig. 2Surgical scars 6 months after robotic single-site surgery (A) and robotic four arms surgery (B).
|
Robotic single-site approach permitted the surgeon to respect the integrity of patient's body image with an easy technique. In fact, the combination of LESS and the robotic system seem to be a promising choice in overcoming the technical difficulties of LESS. This technique was firstly proposed by Mereu et al. [15] in endometrial cancer, where it appears to be a safe and relatively feasible procedure. Subsequently, we conducted a double institution case-control study comparing the surgical results of RSSH and laparoscopic single-site hysterectomy in early endometrial cancer [16]. In this study, we drew the conclusion that few differences exist between the two procedures in terms of operative time, EBL and conversion/complication rates and underlined that the real advantage of the robotic system is the annulment of the conflict between the instruments. In both surgical techniques, we preferred to close the vagina through the vaginal passage. This choice allows us to reduce the chances of dehiscence of the vaginal cuff to near zero, as already reported in the literature [17], and allows us to reduce costs by not using the robotic needle holder.
RSSH seems to be a safe technique that can be learned by skillful surgeons in as less number of cases. In fact, Paek et al. [18] suggested that the learning curve and proficiency could be achieved after 40 cases in LESS, while with robotic single-site platform, Cela et al. [19] suggest, even if the number of patients analyzed in this study was small, that after a learning curve phase of about 10 cases, the surgeon may achieve a high level of competence. Our present study reports similar figures concerning RSSH; however, it is the first report in literature comparing this cohort with a control group of multiport robotic hysterectomies. We did not observe any difference between the two techniques in terms of surgical and oncological outcomes. In fact, the difference statistically significant of blood loss between RSSH group and RMPH group was not clinically significant and also because in the RMPH group there were more pelvic lymphadenectomy and adhesiolysis that may have led to greater blood loss. Moreover, blood transfusions performed in two patients in RMPH group were due to because the patients were suffering from moderate anemia before surgery and not to blood loss during surgery. In the RMPH, hospitalization was strongly influenced by the prolonged hospital stay: a patient had a median length of stay of 7 days due to fever. In fact, without this patient, the median length of stay was 2 days, which is the same compared to the RSSH group. Although the median follow-up for the RSSH group is still less than 5 years of survival, according to our oncological results, all patients in this group are alive without disease similar to the other group where the median follow-up is greater.
We did not observe any clinically significant difference between the two groups, even among patients with BMI >30 kg/m2 (26% in the RSSH group and 34% in RMPH group). Although few patients, in our experience, it seems that RSSH can also be performed in patients with BMI >30 kg/m2 as reported recently in the literature [20].
In an era of shrinking reimbursements and added financial pressures on both hospitals and insurance providers, medical surgical technology have emerged as a major driving force in increasing health-care costs. Comparative cost studies demonstrate almost 2-fold higher costs for robotic-assisted versus laparoscopic techniques (€4,067 vs. €2,151, p<0.05) after controlling age, BMI, and uterine weight [21]. Even after adjusting for variables such as surgeon's experience and hospital characteristics, Wright et al. [22] found robotic hysterectomy to be $1,291 more costly than laparoscopic approaches (95% CI, $985 to $1,597). However, after calculating for societal/productivity losses, robotic approaches demonstrate cost savings over open approaches, with mean costs of $8,212 versus $12,943 (p=0.0001), respectively [23]. Moreover, Lau et al. [24] showed that the overall hospital costs were significantly lower for robotics compared with laparotomy or laparoscopic even when acquisition and maintenance cost were included (Can$8,370 compared with Can$10,368, p=0.001). In our study, we observed a decrease of the total costs of about $2,591.09 per patient for the RSSH than the RMPH group. In consideration that the rate of complications, the days of hospitalization and return to normal activities were very similar between the two groups, this difference is mainly explained by the decrease in the cost of the disposable robotic single-site equipment by approximately 12% compared to robotic multiport surgery. Certainly, one of the greatest limitations of the single-site platform is that the semi-flexible robotic instruments are not currently capable of articulation as in multiport robotic surgery, and the cannulas are rather long. This means that there are fewer degrees of freedom than with multiport robotic surgery and a very small distance between the instrument and the uterus. However, limitations of this study were the retrospective nature of the data collection for the historical cohort and that the validity of charge comparisons depends upon the charge structure of the health system.
In conclusion, single-site port robotic surgery is still very much in its infancy and the development of the existing technology will be capable to impose this kind of technique in everyday practice for gynecologic oncology surgical practice, even if further studies are eagerly warranted to confirm such benefits.
 XML Download
XML Download