

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine serous carcinoma (USC) represents a distinct aggressive variant of endometrial cancer closely resembling ovarian serous cancer. USC accounts for 5% to 10% of all endometrial cancers [123] but represents 25% to 40% of endometrial cancer related deaths and 50% of endometrial cancer related recurrences [12345]. Several retrospective studies suggested a beneficial role for adjuvant chemotherapy in the majority of patients diagnosed with USC [678].
There are still unresolved questions regarding optimal adjuvant therapy of patients diagnosed with USC. Given the aggressive nature of this disease and its propensity for systemic spread, adjuvant chemotherapy has become the standard adjuvant therapy in patients with USC. However, the question remains whether radiation therapy will provide any additional survival benefit when combined with chemotherapy. The evidence in the literature to answer this question is limited. Phase II trials have demonstrated that combined adjuvant chemotherapy and radiation is well tolerated in USC patients [91011]. In one retrospective study of patients with stage I-IV USC, use of radiation therapy and chemotherapy containing paclitaxel was associated with longer progression-free survival [8]. However, these data were not compared to those who received chemotherapy alone and were also limited by small sample size. The objective of this study was to assess the impact of pelvic radiation on outcome (overall survival [OS] and disease-specific survival [DSS]) in patients with USC who also received adjuvant chemotherapy using the population database of the Surveillance, Epidemiology, and End Results (SEER) program.
MATERIALS AND METHODS
Women with a diagnosis of USC were identified using SEER data from 2000 to 2009. Only women who were known to receive chemotherapy during their primary treatment were included. Other inclusion criteria included patients who were treated with surgery with at least hysterectomy with or without lymphadenectomy, serous histology (International Classification of Diseases, 3rd edition [ICD-3] codes 8460/3, 8461/3, and 8441/3), known age, known lymphadenectomy status and lymph node status (not done, negative, or positive) at the time of primary surgical treatment, known radiation status (received no radiation, pelvic radiation with or without brachytherapy) and active follow-up. Patients were grouped into two cohorts: those who received chemotherapy only (CT) and those who received both chemotherapy and pelvic radiation therapy +/– brachytherapy (CT_RT). Patients were considered to be included in the radiation group if they received external beam radiation +/– brachytherapy. Patients who received chemotherapy and brachytherapy alone were excluded. Information was not available on type of chemotherapy regimen or number of cycles received.
The SEER database provides information on the disease stage based on clinical, intraoperative, and pathological findings. Stage III and IV in this manuscript represent the actual The International Federation of Gynecology and Obstetrics (FIGO) stage. Stage I and II contain a combination of cases with actual FIGO stage (I and II) and “apparent stage” (I and II). Here, apparent stage I-II was determined for patients without staging lymphadenectomy but other known operative, and pathology findings sufficient to identify the extent of disease based on FIGO staging 2009 recommendations, as previously reported [1213]. When detailed information on extent of disease was not available, those cases were classified as unknown stage.
The primary end point of the study was outcome (OS and DSS) among those who received radiation therapy compared to those who did not. The secondary endpoint was to assess the impact of radiation on outcome in subset of patients stratified by stage (I–IV).
Patients were categorized in the lymphadenectomy group if any lymph nodes were recovered. Further, patients who underwent lymphadenectomy were divided into two groups based on the number of lymph nodes reported (<10 and ≥10 nodes). The 10 lymph nodes cutoff was chosen based on the Gynecologic Oncology Group (GOG) criteria for adequate lymphadenectomy. Demographic, clinicopathologic, treatment, and survival information were extracted using the “Case Listing” option of the SEER Stat software.
Associations between categorical covariates were assessed using chi-square tests or Fisher Exact test, while the Welch t-test was used to assess group differences for continuous covariates. A two-sided p-value of ≤0.05 was considered statistically significant. Survival curves were estimated using the Kaplan-Meier method. All persons alive were censored when the outcome of interest was OS; and deaths due to all causes other than endometrial cancer were censored in addition to all who were alive when DSS was analyzed. Cox proportional hazards regression was used to identify independent predictors of survival. Factors entered in the multivariable model included age at diagnosis, race, stage of disease, extent of lymphadenectomy (no lymphadenectomy vs. <10 lymph nodes removed vs. ≥10 lymph nodes removed) and adjuvant radiation therapy. R 3.1.1 (Vienna, Austria) was used to analyze the data.
RESULTS
Eighteen hundred and thirty-eight women with USC met the inclusion criteria. All patients received chemotherapy. Median age at diagnosis was 66.6 years. Of these patients, the majority, 1,272 (69%) received adjuvant CT and only 566 (31%) received external beam radiation+/– brachytherapy (CT_RT). Seventy percent of the patients underwent staging lymphadenectomy (1,291/1,383). The majority of patients had advanced stage disease (68%). Patients’ characteristics comparing CT and CT_RT groups are listed in Table 1.
Table 1
Demographic and clinical characteristics of patients with uterine serous carcinoma who received chemotherapy stratified by adjuvant radiotherapy (n=1,838)

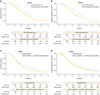
Kaplan-Meier analysis demonstrated significant improvement in OS (median: 50 months vs. 31 months; 5-year 45% vs. 30%; p<0.001) and DSS (77 months vs. 48 months; 5-year 54% vs. 44%; p<0.001) in CT_RT compared CT groups respectively (Fig. 1). In stage I, there was no difference in OS (median: not reached for both; 5-year 72% vs. 72%; p=0.63) and DSS (median: not reached for both; 5-year 82% vs. 81%; p=0.71) between CT_RT and CT groups respectively (Fig. 2A, B). Whereas in stage II, CT_RT was associated with longer OS (median: not reached vs. 44 months; 5-year 72% vs. 47%; p=0.05) and trend toward longer DSS (median: not reached for both; 5-year 79% vs. 59%; p=0.13) compared to CT (Fig. 2C, D). In patients with stage III, CT_RT was associated with improved OS (median: 42 months vs. 32 months; 5-year 38% vs. 27%; p=0.002) and DSS (median: 52 months vs. 42 months; 5-year 47% vs. 39%; p=0.026) when compared to CT (Fig. 3A, B). On the other hand in stage IV, CT_RT was associated with longer OS (median: 23 months vs. 21 months; 5-year 19% vs. 13%; p=0.03) but there was no difference in DSS (median: 30 months vs. 25 months; 5-year 25% vs. 25%; p=0.40) compared to CT (Fig. 3C, D).
Fig. 1
Kaplan-Meier curves for overall survival (A) and disease-specific survival (B) in patients with uterine serous carcinoma who received chemotherapy stratified by pelvic radiation.
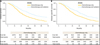
Fig. 2
Kaplan-Meier curves in overall survival and disease-specific survival in patients with early stage (I–II) uterine serous carcinoma (USC) who received chemotherapy stratified by pelvic radiation. Overall survival (A) and disease-specific survival (B) in stage I USC. Overall survival (C) and disease-specific survival (D) in stage II USC.
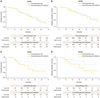
Fig. 3
Kaplan-Meier curves in overall survival and disease-specific survival in patients with advanced stage (III–IV) uterine serous carcinoma (USC) who received chemotherapy stratified by pelvic radiation. Overall survival (A) and disease-specific survival (B) in stage III USC. Overall survival (C) and disease-specific survival (D) in stage IV USC.
In multivariable analysis adjusting for age, race, stage and extent of lymphadenectomy, adjuvant radiation therapy was associated with significant improvement in OS (hazard ratio [HR], 0.79; 95% CI, 0.67 to 0.92; p=0.003) and DSS (HR, 0.84; 95% CI, 0.70 to 1.0; p=0.05) (Table 2) for the entire cohort.
Table 2
Multivariate analysis in patients with uterine serous carcinoma who received adjuvant chemotherapy
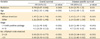
In subset multivariable analysis when adjusting for age, race, and extent of lymphadenectomy, adjuvant radiation therapy was not associated with improved outcome for stage I OS (HR, 0.87; 95% CI, 0.52 to 1.46; p=0.59) and DSS (HR, 0.80; 95% CI, 0.41 to 1.53; p=0.49), stage II OS (HR, 0.90; 95% CI, 0.33 to 2.45; p=0.83) and DSS (HR, 1.17; 95% CI, 0.32 to 4.29; p=0.82), and stage IV OS (HR, 0.91; 95% CI, 0.68 to 1.21; p=0.50) and DSS (HR, 0.99; 95% CI, 0.72 to 1.38; p=0.96). On the other hand, adjuvant radiation therapy was associated with improved outcome OS (HR, 0.75; 95% CI, 0.59 to 0.96; p=0.02) and DSS (HR, 0.78; 95% CI, 0.59 to 1.0; p=0.07) for stage III.
DISCUSSION
In this large cohort of patients diagnosed with USC using SEER program, we demonstrated that combined treatment modality with chemotherapy and radiation therapy is associated with improved OS and DSS compared to chemotherapy alone. The impact of pelvic radiation on outcome was evident only in patients with stage III disease. We did not see a difference in outcome in early stage (I–II) and stage IV USC between those who received chemotherapy alone and those who received chemotherapy and radiation therapy. Patients who received combined radiation and chemotherapy were less likely to have stage IV disease and more likely to have lymphadenectomy compared to those who received chemotherapy alone leading to unbalanced groups. However, our findings remained consistent in subset analysis of each stage and in the multivariable models adjusting for these confounders.
NCCN guidelines recommend systemic therapy for patients with USC with any myometrial invasion. This is consistent with multiple retrospective studies [67814151617]. Controversy exists when USC is non-invasive or confined to a polyp where observation, radiation, or chemotherapy with or without radiation listed as possible acceptable treatments per the NCCN guidelines. Chemotherapy has now become the standard adjuvant treatment modality in USC. However, the question is whether adding radiation could provide better disease control and survival advantage. Given the rarity of this aggressive tumor, this question has not been addressed prospectively or retrospectively in a comprehensive fashion in this patient population. Our study suggests a survival benefit with the addition of pelvic radiation therapy in patients diagnosed with USC.
Randomized data in patients with USC is limited. In patients with advanced stage endometrial cancer, data from GOG 122 showed superiority of systemic chemotherapy over abdominal radiation. However, loco-regional recurrence was higher in the chemotherapy arm, which raises the question regarding the benefit of the combined adjuvant approach and its impact on locoregional control and outcome in advanced stage disease [18]. GOG 122, was not powered enough to assess the impact of adjuvant chemotherapy versus whole abdominal radiation in patients with USC (n=83). GOG 258 is evaluating the role of tumor directed radiation in patients with advanced stage endometrial cancer. The trial randomizes patients to tumor directed concurrent chemoradiation followed by four cycles carboplatin and paclitaxel chemotherapy versus six cycles of carboplatin and paclitaxel alone. The trial, which has not yet been presented, accrued slightly more than 100 patients with USC.
Multi-institutional retrospective studies support the use of radiation and chemotherapy for advanced stage endometrial cancer. Alvarez Secord et al. [19] in the retrospective study of 356 patients with advanced stage endometrial cancer showed the superiority of combined radiation and chemotherapy compared to single modality treatment following surgery. However, this study included all histology types and was limited by an imbalance between the treatment groups [19]. More recently Secord et al. [20] investigated the impact of three adjuvant treatment approaches (chemotherapy, radiation, and combined chemotherapy with radiation) in 256 patients with optimally debulked stage IIIC endometrial cancer in a multi-institutional study. In that study, treatment with adjuvant radiation alone or combined chemotherapy and radiation therapy was superior to chemotherapy alone. Again this study included patients with different histologic types with only 25 patients (10%) with serous histology [20].
In USC, a retrospective study from Mayo investigated the outcome of uterine papillary serous carcinoma (UPSC) patients with advanced stage disease (III–IV) and reported a significant improvement in survival associated with aggressive surgical cytoreduction and adjuvant chemotherapy [15]. Unfortunately, this study did not address the role of radiation. Similarly in a retrospective study from Taiwan that included 67 patients with advanced stage USC, combined radiation and chemotherapy was a significant predictor of progression-free survival and OS [16]. Given the lack of data on the role of adjuvant radiation along with chemotherapy in this unique patient population, our data showed that there is a survival advantage associated with radiation in patients with stage III USC who received chemotherapy. Our data also suggests a trend towards benefit in stage II patients, which did not reach statistical significance, most likely due to the small number of stage II patients in our cohort. Prior phase II trials of combined adjuvant treatment modality showed that this approach is well tolerated in USC patients.
On the other hand, our finding does not support use of pelvic radiation along with chemotherapy in patients diagnosed with stage I USC. This is in line with previously published retrospective data reporting excellent survival outcomes with chemotherapy alone or in combination with brachytherapy [6721]. In contrast to our study, these studies did not compare the outcomes of patients receiving the combined modality approach to chemotherapy alone.
Patients with stage IV USC also did not benefit from pelvic RT in our analysis and further investigation is warranted as to the optimal systemic therapy for these patients. Distant metastasis in patients with stage IV are generally not covered with radiation therapy, which can explain the lack of survival benefit of radiation therapy in this group of patients.
Interestingly, patients with early stage disease with positive cytology or washing had worse outcome compared to those with negative cytology. These data support routine pelvic cytology as a part of surgical staging of UPSC consistent with FIGO recommendations. Prior studies report conflicting results in patients with endometrial cancer with positive cytology but did not investigate its prognostic significance specifically in UPSC [222324]. Other predictor of outcome was extent of lymphadenectomy. The impact of extent of lymphadenectomy is consistent with the findings of our prior study [25], which further supports the survival advantage of extensive lymphadenectomy even in patients who received postoperative chemotherapy with or without radiation.
Another interesting finding of this study is that African American race was a significant predictor of worse OS and DSS in the multivariate analysis. This finding held up in the subset analyses of both early stage and advanced stage disease. Prior studies have reported controversial results [262728]. Al-Wahab et al. [26] in a single institutional study of USC reported no difference in outcome between white and African American patients with USC when they receive equal treatment at tertiary centers. In our study, African American race was a predictor of worse survival in settings where all patients received surgical treatment followed by chemotherapy with or without radiation therapy. In our study, African American race was a predictor of worse survival in settings where all patients received surgical treatment followed by chemotherapy with or without radiation therapy. This finding raises the question of the presence of potential biologic factors that could lead to racial differences in cancer outcomes.
Our analysis was limited by a lack of information on physician subspecialty, central pathologic review, recurrences, treatment of recurrence, socioeconomic status, and comorbidities. This study was limited to patients known to have received chemotherapy and it is unclear how many women were not included because their chemotherapy status was unknown when they actually received chemotherapy. Further SEER dataset lacked information on chemotherapy regimen and number of cycles. We also did not have information on the extent of nodal disease (pelvic vs. para-aortic), extent and reasons for pelvic radiation therapy. However, the strength of this study is that this is the largest study evaluating the impact of radiation in a large cohort of USC patients who were surgically staged and received chemotherapy. Because the SEER cancer registries are compiled from representative regions throughout the country, including large and small hospitals, as well small community practices, the results from this population-based study can be generalized to the entire United States population. Therefore, the risk of referral or access to care biases, which can arise when racial disparities are studied using large institutional data, are reduced in this study.
In conclusion, in this large cohort of patients with USC who received surgical treatment and chemotherapy, we demonstrated that radiation therapy has a significant impact on OS and DSSs of patients with stage III USC but not for those with early stage or stage IV USC. Therefore, combined modality treatment with both chemotherapy and radiation therapy should always be considered in patients diagnosed with stage III USC if possible. Future randomized trials are needed to compare the impact of combined adjuvant therapy versus single modality treatment on survival outcomes in this patient population. Furthermore, positive cytology was a significant predictor of poor outcome and therefore it should still be a part of surgical staging, especially in patients with early stage disease.
 XML Download
XML Download