

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Primary vaginal cancer is a rare malignancy, accounting for 1% to 2% of all gynecologic malignancies. According to the annual report on cancer statistics in South Korea in 2012, the annual incidence of vaginal cancer accounts for 0.1% of the all-cancer registry, with a 5-year incidence of approximately 240 patients, which is lower than the reported data [1]. Therefore, most studies of primary vaginal cancer are small due to the rarity of the disease.
To treat vaginal cancer, surgical options can be considered for highly selected small and localized early-stage patients. Radiotherapy (RT) with or without chemotherapy is a treatment of choice for most primary vaginal cancer patients. Additional chemotherapy is often used by extrapolating cervical cancer data, yet no randomized trial has compared RT alone and concurrent chemoradiotherapy (CCRT). Recently, the National Cancer Data Base of the United States has reported the results of the study of the largest population of primary vaginal cancer patients and provided survival data and prognostic factors of data for over 8,000 patients, which revealed the superiority of CCRT over RT alone in the treatment of primary vaginal cancer [2]. However, detailed data were significantly missing, such as the purpose of chemotherapy or RT (inductive or definitive) and the toxicity profile. Moreover, though this study was designed to deal with definitive RT, patients who had undergone lymphadenectomy were included.
To overcome the limitations of previous studies of primary vaginal cancer due to the rarity of the disease, the Korean Radiation Oncology Group (KROG) performed a multi-institutional retrospective study, the results of which are reported herein.
MATERIALS AND METHODS
1. Patients and tumor characteristics
This multicenter retrospective study was conducted on primary vaginal cancer patients treated with definitive RT with or without chemotherapy from June 1976 to November 2011 in nine institutions approved by KROG (KROG, 12-09). Patients with distant metastasis were excluded, except patients who had para-aortic lymph node metastasis, as those could be covered by the extended pelvic RT field. Patients with a history of curative excision, who were in the Tis stage, or who had a histology of vaginal melanoma were also excluded. Patients were diagnosed as vaginal cancer in case where there was no evidence of recurrence of cervical/endometrial cancer for more than 10 years or when histologic subtypes were different from the two diseases. This study was approved by the Institutional Review Board of each of the included institutions.
A total of 152 patients in nine institutions who satisfied the inclusion criteria were identified. Of these, 11 patients with incomplete RT or an RT dose ≤ 50.4 Gy to the vagina were excluded. Three patients whose follow-up period was less than four months were also excluded. Finally, 138 patients were evaluated for the survival analysis. The patient, tumor, and treatment characteristics are shown in Table 1. The median age was 61 years (range, 30 to 84 years). Seven patients had a history of cervical cancer, and 13 had carcinoma in situ (CIS) before vaginal cancer. Fifty-five patients had undergone hysterectomy, 22 of them for malignancy (seven for cervical ca, one for endometrial cancer, one for malignant mixed Müllerian tumor, and 13 for CIS) and 33 for various benign diseases such as uterine fibroids or pelvic inflammatory disease. One patient had a pelvic RT history because of cervical cancer. All the patients underwent a thorough gynecological examination at the time of their diagnosis, with chest X-ray for 90% of the patients, cystoscopy for 59%, colonoscopy for 70%, a pelvic computed tomography (CT) scan for 54%, a pelvic magnetic resonance imaging scan for 62%, and a positron emission tomography-CT scan for 28%. Generally, the size was measured by imaging studies if available, or by gynecological exams.
Table 1
Patient, tumor, and treatment characteristics

Eighty-six percent of the patients were diagnosed with squamous cell carcinoma (SqCC), and 24% had tumors larger than 4 cm. The human papillomavirus (HPV) status of the tumor was available in 27 patients, and 17 (63%) of those were HPV-positive. The HPV-positive tumors were all SqCC.
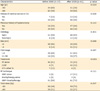
When the patients who had undergone RT alone were compared with the CCRT group (n=127), the RT alone group showed a stronger history of cervical cancer or CIS, and more patients received the treatment before the year 2000 (Table 2). Moreover, in the comparison of the patients treated before the year 2000 and after 2000, there were more older patients, more large tumors, and more CCRT procedures performed on the patients treated after 2000, whose total dose was also lower (Table 3).
Table 2
Patients characteristics according to the treatment (n=127)
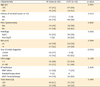
Table 3
Patients characteristics according to the year of diagnosis
2. Treatment
Eighty-one percent of the patients had undergone both external beam radiotherapy (EBRT) and brachytherapy; 16%, EBRT alone; and 3%, brachytherapy alone. The pelvic RT field of the 134 patients who had undergone EBRT basically included their entire vagina and their pelvic lymph nodes, and 53 of them were selected to undergo extended field pelvic RT that included their inguinal lymph node or para-aortic lymph node regions. The median dose for the pelvis was 46 Gy (range, 39.6 to 54 Gy). Boost doses were given to 49 patients for gross primary tumor, the parametrial region, or lymph nodes. Among the node-positive patients (n=34), 27 underwent boost irradiation of their grossly enlarged lymph nodes.
For the intracavitary brachytherapy, low-dose rate from a cesium-137 radioactive source (median dose, 40.2 Gy; range, 30 to 65.2 Gy) was used for 35 patients in two hospitals, and high-dose rate via iridium-192 (median dose, 30 Gy; range, 10 to 50 Gy), for 80 patients in seven hospitals. Vaginal cylinders or Fletcher-Suit-Delclos colpostats were used for brachytherapy. The dose prescription point was 0.5 or 1.0 cm in depth to the surface of the vaginal mucosa to cover the gross residual tumor after EBRT, which was made upon clinician's decision.
3. Statistical analysis
The survival durations were calculated from the first day of the initial treatment. Overall survival (OS) and cancer-specific survival (CSS) were defined as the time to death from any cause and the time to death from vaginal cancer. Loco-regional recurrence-free survival (LRFS) and progression-free survival (PFS) were defined as the time to the loco-regional and overall recurrence, respectively. The Kaplan-Meier survival graphs and statistical differences were presented using the log-rank test. A Cox proportional hazard model was used for the multivariate analysis, and the variables showed a p-value <0.2 in the log-rank test. To find predictors of grade 3 or 4 late toxicity, logistic regression analysis was used. All the statistical analyses were carried out using SPSS ver. 22 (IBM Co., Armonk, NY, USA). A p<0.05 was considered statistically significant.
RESULTS
1. Treatment outcome
The median follow-up time of the survivors was 77.6 months (range, 4.4 to 426.1 months). The median survival time was 46.9 months (range, 4.3 to 426.1 months). Twenty-seven patients (20%) died from vaginal cancer during the follow-up period, and 25 (18%) died from other causes. The 5-year OS, CSS, and PFS rates were 68%, 80%, and 68.7%, respectively. The 5-year LRFS rate was 74%. The 5-year OS rate in stage I of the International Federation of Gynecology and Obstetrics (FIGO) staging system was 75.4%; in stage II, 68.8%; in stage III, 68%; and in stage IV, 47%. The 5-year CSS rate in stage I was 85%; in stage II, 83.6%; in stage III, 74.5%; and in stage IV, 69.2%. The 5-year PFS rate in stage I was 78.9%; in stage II, 66%; in stage III, 52.5%; and in stage IV, 65.2%.
The prognostic factors of the OS and the CSS, as well as of the 5-year survival rate, significantly differed. In the multivariate analysis, an age above 60 and treatment after the year 2000 were statistically significant for the OS. In contrast, the FIGO stage and prior hysterectomy were associated with the CSS (Table 4). In the same analysis, the year of the initial diagnosis and the FIGO stage were found to be related to the PFS, and the year of the initial diagnosis, to the LRFS.
Table 4
Prognostic factors for survival outcome of primary vaginal cancer

CCRT, concurrent chemoradiotherapy; CIS, carcinoma in situ; CSS, cancer-specific survival; EBRT, external beam radiotherapy; FIGO, International Federation of Gynecology and Obstetrics; ICT, induction chemotherapy; LRFS, loco-regional recurrence-free survival; OS, overall survival; PFS, progression free survival; RT, radiotherapy; SqCC, squamous cell carcinoma.
*Log-rank test. †Cox proportional hazard model.
Distant metastasis occurred in 19 patients (13.7%). The most common sites of the metastases were the lung (in five patients) and the para-aortic lymph node (in five patients), followed by the supraclavicular lymph node (in four patients). Two patients each had liver, cervical lymph node, peritoneum, and brain metastases, and one patient had bone, abdominal wall, and mediastinal lymph nodes.
2. Subgroup analysis of the HPV-tested patients
In the patients whose tumor HPV status was available (n=27), no statistically significant difference was found in all the outcomes. However, the patients with HPV-positive tumors all showed trends toward better survival outcomes, especially in the LRFS (5-year OS: 68.8% for the HPV-positive patients vs. 44.4% for the HPV-negative patients, p=0.406; 5-year CSS: 82.4% vs. 74.1%, p=0.748; 5-year PFS: 81.6% vs. 64.8%, p=0.386; and 5-year LRFS: 93.3% vs. 77.8%, p=0.219).
3. Complications
The toxicity profiles of the treated patients are listed in Table 5 and were recommended to be graded according to the Common Terminology Criteria for Adverse Events ver. 4.0. Sixteen patients (12%) had grade 3 or 4 acute toxicity; 12 (9%), grade 3 or 4 acute skin toxicity; one (1%), grade 3 acute gastrointestinal (GI) toxicity; and three (2%), grade 3 acute genitourinary toxicity. Twelve patients (8%) showed late toxicity. Grade 3 or 4 late GI toxicity occurred in nine patients (7%), and grade 3 or 4 genitourinary complications, in eight patients (6%). Grade 3 or 4 late skin toxicity developed in three patients (2%). Prognostic factors for severe toxicity (age, prior hysterectomy, histology, tumor size, year of initial diagnosis, FIGO stage, treatment, RT technique, and total dose) were evaluated by logistic regression. The result showed that a higher FIGO stage (I or II vs. III or IV) (odds ratio [OR], 4.153; 95% CI, 1.145 to 15.056; p=0.03), and an over 4 cm tumor size (OR, 4.044; 95% CI, 1.189 to 13.756; p=0.025) were significantly related to the risk of grade 3 or 4 late toxicity.
Table 5
Toxicity profiles in patients treated for primary vaginal cancer

DISCUSSION
This study presents the results of treatments of primary vaginal cancer with definitive RT in multiple institutions in Korea for 35 years. The presented CSS outcomes were comparable to or higher than those in recently reported data [345]. The results of this study showed that the prognostic factors of the OS (the age and the year of the initial diagnosis) and the CSS (prior hysterectomy and the FIGO stage) significantly differed. Because many deaths were unrelated to vaginal cancer, the CSS rather than the OS represented the survival outcome after the treatment of primary vaginal cancer. Therefore, the authors focused on the CSS rather than the OS in the interpretation of the results.
In this study, the FIGO stage was strongly associated with the CSS and the PFS in the multivariate analysis, as expected [36]. Additionally, prior hysterectomy was related to better CSS. It has been acknowledged that a number of vaginal neoplasms develop after hysterectomy [78]. In the recent study of Daling et al. [9], they also found that prior hysterectomy was a risk factor of vaginal cancer in women with no history of anogenital cancer. The data are consistent with the results of Chyle et al. [10] and Tran et al. [4], which showed the relationship between prior hysterectomy and the vaginal cancer survival outcome. Although the relationship was inconclusive, the researchers attributed the better survival in the prior hysterectomy group to early diagnosis and the smaller tumors due to the absence of the uterus and the lower amount of vaginal substrates.
Although the tumor size is known as an important prognostic factor of the survival of vaginal cancer patients, its accurate measurement is difficult without surgery due to the anatomical difficulties [11]. Therefore, it is difficult to apply an accurate tumor size to the prediction of the survival outcome in a clinical setting without surgical resection in the clinical setting. The data from the univariate analysis in this study also showed better disease control in small tumors (≤4 cm), as in other studies [23], but they were insignificant in the multivariate analysis in this study.
The results of this study that were difficult to interpret were that the patients treated after the year 2000 had much worse LRFS, PFS, and OS rates and tended to have worse CSS rates. Although such results remained significant after they were adjusted based on other factors in the multivariate analysis, increased surgery in the treatment of early-stage vaginal cancer and the use of neo-adjuvant chemotherapy were speculated to have facilitated curative resection in the previously unresectable cases. The reported results of the National Cancer Data Base and Surveillance, Epidemiology, and End Results data analysis after the 1990s showed better survival outcomes with surgery than with definitive RT, but also inherent selection biases [1112]. Therefore, there could have been trends toward increased surgical resection before considering definitive RT in early-stage vaginal cancer. As seen in Table 3, there were older patients and patients with larger primary tumors in the group treated after the year 2000. Several surgical series showed biases in the selection of surgical candidates and more unfavorable cases treated with RT [131415].
Another result of this study that differed from that of other studies was that the CCRT did not show a survival benefit and instead, showed an inferior survival outcome in the CCRT group [2]. Therefore, the RT-alone group and the CCRT group were compared, as shown in Table 2, and the comparison revealed trends toward more non-SqCC in the CCRT group and the treatment of more patients after the year 2000. Therefore, selection biases were speculated in the decision-making on the vaginal cancer treatment modality in Korea.
Research on the effect of the tumor HPV status on vaginal cancer survival is still in its early stage mainly due to the rarity of vaginal cancer, but there is a presumption that the tumor HPV status in vaginal cancer would also contribute to the cancer development or the treatment response, based on the studies of head and neck cancer as well as of cervical cancer [1617]. Sinno et al. [18] examined the HPV status in 60 cases of vaginal cancer, and found that 75% were HPV-positive and 25% were HPV-negative. The unadjusted OS rates in the HPV-positive patients were 57.4% and 35.7% for the HPV-negative patients, but they were statistically insignificant (p=0.243) [18]. This study included 27 patients with HPV test results, 63% of whom were HPV-positive, and their survival rates showed no statistically significant difference. That might have been due to the small number of patients in the performed studies, because the data showed a trend toward a better survival outcome in HPV-positive patients. Therefore, a further study with a sufficient number of patients is needed.
Regarding acute toxicity, 12% of the patients experienced a severe (grade 3 or 4) acute complication, lower than in other studies (24% to 40%). However, the late toxicity result was comparable to that of other studies, in that 8% of the patients had a grade 3 or 4 late complication [5101920]. However, as Hegemann et al. [19] stated, clinicians grade toxicities differently, which makes it difficult to directly compare the results of various studies. However, the toxicities are still considerable. Therefore, based on these data, toxicities should be considered during treatment, especially late toxicities, and special attention should be paid to the characteristics of each tumor. The results of this study showed that a higher FIGO stage and a larger tumor could significantly predict severe late toxicity, as mentioned in some previous studies [34]. Other researchers have reported the predictors of complications as a higher RT dose [2122], pelvic lymphadenectomy [10], a higher FIGO stage, and a smoking history [3]. As mentioned, the FIGO stage is also a critical risk factor of the disease recurrence and worse CSS, as well as a predictor of severe late toxicity. Therefore, especially in the advanced stage, more precise RT such as intensity-modulated RT or brachytherapy planning with three-dimensional imaging should replace conventional RT to enhance the treatment outcome and to reduce the toxicity.
This multicenter study revealed that the institutions had heterogeneous treatment policies. Furthermore, the obtainable data were limited, such as the location of the tumor, tumor markers, detailed RT technique, and salvage treatment after recurrence, because they were lacking in some institutions. However, a multicenter study on this rare malignancy was inevitable to accrue analyzable data, because a single-institution study could not provide useful prognostic factors of survival due to the small number of patients, except for large institutions, and the study of the national database provided few of the important data. An attempt was made to enhance the homogeneity of the data, especially on the treatment schemes, by strictly excluding cases of prior excision before RT and Tis lesions, which were included in previous studies [210].
In conclusion, a survival outcome comparable to or higher than the historical data and moderate toxicities in the patients with primary vaginal cancer were shown, and revealed that a lower FIGO stage and prior hysterectomy are favorable prognostic factors. The FIGO stage and the tumor size were related to higher severe toxicity. Therefore, individualized precise treatment of advanced-stage vaginal cancer is imperative. In the patients whose tumor HPV status was available, 63% had an HPV-positive tumor. No relationship was found between the patients with HPV-positive and -negative tumors, but there was a trend toward better local control in the HPV-positive patients. Therefore, a further study on HPV in vaginal cancer is needed.
 XML Download
XML Download