

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Seat belts have been shown to provide protection in motor vehicle crashes, particularly in preventing ejection from the vehicle. However, the seat belt itself can be a factor for injury. The ''Seat Belt Syndrome'', first described by Garrett and Braunstein [1] in 1962, and recently described by Newman et al. [2] as the ''lab belt complex'', refers to the spectrum of injuries including; intestinal tears, perforations; and lumbar distractions, dislocations, and lumbar fractures. Several cases of appendiceal injuries resulting in posttraumatic appendicitis have been reported, but appendiceal transection associated with seat belt restraints is extremely rare [3]. Therefore, this report presents a 23-year-old man with manifestations of generalized peritonitis within a few hours after a motor vehicle crash with seat belt restraint, in whom exploratory laparotomy revealed the appendiceal transection.
CASE REPORT
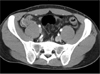
A 23-year-old man presented to the Emergency Department several tens of minutes after a head-on motor vehicle collision. He was hemodynamically stable and complained of lower abdominal discomfort. Physical exam revealed ''seat-belt sign'' ecchymosis along the 3-points of safety belts, especially the right lower quadrant with mild tenderness (Fig. 1). A small amount of fluid collection in the pelvic cavity was observed on FAST (Focused Assessment in Sonography for Trauma), which did not increase after 30 minutes. An abdominal computed tomography scan also showed a small amount of fluid collection in the pelvic cavity without pneumoperitoneum or extravasation of contrast (Fig. 2). So we decided to observe him closely in the intensive care unit.
The patient developed severe pain in the periumbilical area as well as the lower abdomen within 8 hours and also presented peritoneal irritation signs on physical exam. He was taken to the operating room immediately without further evaluation. Exploration of the abdomen revealed about 500 mL of blood in the abdominal cavity and 7-cm tearing of the distal ileum mesentery (Fig. 3). The appendix was transected completely at its proximal portion and the free distal portion of the transected appendix was found in the pelvic cavity (Fig. 4). Appendectomy of the remaining appendix and mesenteric repair were performed. He had an uneventful postoperative course except surgical wound infection and was discharged 15 days after operation.
DISCUSSION
Before the use of seat belts, intra-abdominal injuries sustained in motor vehicle crashes primarily involved solid viscera such as liver and spleen. Serour et al. [4] have claimed that direct appendiceal injury is generally coexistent with other intra-abdominal organ injuries, and that the appendix is very rarely affected by direct trauma owing to its high mobility and small dimensions. The mechanisms for appendiceal injury in patients wearing seat belt is probably related to the sudden increase in intraluminal pressure with displacement of feces and gas into the appendix and mucosal injury, displacement of mobile viscera with traction at fixed points, or direct traumatic injury [5]. These mechanisms may have accounted for the observed appendiceal transection and mesenteric tears in this patient.
Appendiceal rupture after blunt trauma is exceedingly rare. Denis reported blunt rupture of the appendix in one of 38 injured patients restrained during automobile accidents [6]. Whether appendiceal rupture occurs as a complication of advanced acute appendicitis or as a consequence of direct blunt abdominal trauma has yet to be fully clarified [7]. In our case, the patient had been asymptomatic before the trauma and there was no histopathologic evidence of advanced acute appendicitis responsible for the subsequent appendiceal rupture.
In a review of reported cases, appendiceal transection presented symptoms between 3 hours and 2 days after the traumatic event. In 1956, Gatewood and Russum [8] reported a case of complete transection of the appendix following blunt abdominal trauma. The patient, a 39-year-old woman involved in a motor vehicle collision, complained of abdominal pain after 3 hours of observation. Use of a seat belt use was not recorded [8]. In 1977, Pillay and Baker [9] reported a 30-year-old man who developed acute abdominal pain 2 days after a blunt severe direct trauma to the abdomen. In 1992, Statter and Coran [10] reported a 5-year-old girl involved in a motor vehicle crash. She was observed in the intensive care unit, and within 8 hours, developed peritoneal signs. In 2013, Moslemi et al. [7] reported a 13-year-old boy with a history of bicycle handlebar injury. In less than 6 hours, he developed generalized peritonitis. It is worthy of note that, the onsets of symptom vary. In this case, relatively rapid development of the symptoms and signs of generalized peritonitis hinted at chemical peritonitis, which was subsequently confirmed by our observations during exploratory laparotomy.
In conclusion, direct appendiceal trauma is a rare event. Direct seat belt injury may be a factor in addition to deceleration forces applied to fixation points of mobile viscera. Physicians caring for victims with blunt abdominal injuries should be suspicious of posttraumatic appendiceal injuries.



 XML Download
XML Download