

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Operation cancellation puts a huge burden on health care providers and negatively affects patients and their families [1]. Operation cancellation has many definitions in the literature [2]. For the purpose of this study, it is defined as cases that appeared in the definitive operative room (OR) list that ultimately were not performed on that day. International estimates of the incidence of operation cancellation vary with country and type of setting and range from 2% to 30% [3].
Reasons for cancellations are vary widely and may be difficult to tackle all at once. Ezike et al. [2] reported 226 causes of operation cancellation in his study. Cancellation can be due to factors related to health care providers and hospital itself or due to patient-related factors. In a study reported by Garg et al. [4], hospital and administration related factors were the main reasons for operation cancellation. Other researchers have reported that patient-related factors were more important [5].
Health care institutions always strive to efficiently utilize their resources. It would be useful for each institution to determine the most common avoidable reasons for operation cancellation and tackle those first. At Jordan University Hospital (JUH), 18,000–20,000 operations are performed annually making operation efficiency a necessity. A growing body of research is being conducted worldwide to characterize the issue of operation cancellation in referral hospitals. In Jordan, however, despite the regional and international recognition of high-quality health care, there have been only 2 studies reviewing the current situation of operation cancellation [67]. To our knowledge, none of those studies attempted to prioritize the reasons for operation cancellation to thereby direct efforts of improvement. Therefore, the aim of this study is to report the rate of and reasons for operation cancellation at a single university referral hospital, and to prioritize areas of improvement.
METHODS
JUH is a university referral hospital with a capacity of 599 beds. There are 14 operating rooms where major and minor operations can be performed. Each surgeon has an assigned day and operative theatre for his elective cases. Emergency cases are listed on an emergency board and are conducted after the elective lists, while urgent cases interrupt the schedule of the next available theatre. Operation lists for elective procedures are prepared and sent to theatres by the preceding afternoon. Listed cases are evaluated in the ward the evening before the surgery by the anesthesia residents who report potentially difficult cases to a consultant anesthetist.
Daily data on the number of scheduled cases and the number of cancellations are collected by an assigned OR nurse and are reported monthly to the office of quality assurance at JUH. These reports were studied retrospectively from August 2012 to April 2016. Data on reasons for cancellation were available starting from January 2014 and were also reported by the assigned nurse who chose the reason from a list of 10 reasons. These reasons were selected based on a previous pilot study that identified the 10 most common reasons for operation cancellation at JUH. Reasons that didn’t match any of the 10 reasons were reported as “others" and were described by the assigned nurse.
The reasons for cancellation can be assigned into 3 groups: patient no-shows, patient-related reasons, and hospital-related reasons. Patient-related reasons included (upper respiratory tract infections [URTI], impaired cardiac function, impaired pulmonary function, high blood pressure, and uncontrolled blood sugar). Hospital-related reasons included (lack of surgical theatre time, incomplete preoperative assessment, shortage of nursing staff, shortage of anaesthesia staff, and equipment or supplies shortage). Rates and reasons for operation cancellation were investigated. A Pareto chart was constructed to identify the reasons of highest priority.
Statistical analyses were performed using IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA) and Pareto analysis was performed using the Pareto tool on the American Society for Quality website.
RESULTS
The overall cancellation rate during the period from August 2012 to April 2016 was 9.31% (6,431 cancelations out of 69,066 scheduled operations). Fig. 1 shows a flow chart of cancellation rates where the highest incidence was during May 2013 due to a nursing strike (19.18%).
Since January 2014, a total number of 4,261 scheduled operations were cancelled for different reasons. Of those, 2,664 were due to patient no-shows (patient were not admitted to the hospital) accounting for 62.52% of cancellations.
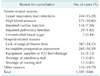
Table 1 presents numbers and rates of cancellation according to the reason after patients were admitted to the hospital.
Other reasons for cancellation included a wide variety of hospital and patient related reasons such as: change of management plan, unavailability of the surgeon, last minute refusal of patients, failure to present consent by the guardian in paediatric patients, fever, patient not fasting, patient not fit for reasons other than those mentioned above, failed intravascular access, death of the patient, and other unspecified reasons.
A Pareto analysis was done to prioritize the identified reasons for cancellation after admission to the hospital according to frequency. The 4 reasons responsible for 83% of operation cancellation after admission to JUH were lack of surgical theatre time (30%), incomplete preoperative assessment (21%), URTI (19%), and high blood pressure (13%) (Fig. 2).
DISCUSSION
Operation cancelation rate at JUH is 9.31%, which is within the literature reported range of cancellation 2%–30% [3].
Cancellation due to patient no-shows (not admitted to the hospital) accounted for about two-thirds of cancellations (62.57%). Although this was the most common overall reason for cancellation in many studies in the literature, including 2 referral hospitals in Jordan, this is an exceptionally high percentage when compared to the rates from the aforementioned studies, 23.0% and 35.6% [67]. Failure to show up for surgery includes patients who made but neither kept nor cancelled a reservation, and patients who cancelled their operation late after operative list distribution.
Patient no-shows for the scheduled surgery is a multifactorial and challenging problem and there has been no consensus among researchers regarding the acceptable cancellation rate due to patient no-shows. For example, the department of health in Australia, set a benchmark of <0.5% for the rate of case cancellation due to patient no-shows [8]. Root causes identifying patient no-shows were not investigated in this study. Potential root causes may include inconvenient date of surgery, patients forgetting about their appointments, or patients’ fear and doubt. At JUH, there is no protocol to remind patients of their appointments. However, to help lower the incidence of patients’ nonattendance, policies should be established by the hospital policy makers to allow dedicated personnel to remind patients through phone calls, text messages, or emails [910]. Reminding patients may improve patient compliance with appointment keeping and seems a logical strategy in our setting where most patients have mobile phones.
The Pareto chart shows that the most common reasons for scheduled operation cancellation after admission were lack of surgical theatre time, incomplete preoperative assessment, URTI, and high blood pressure. It appears that these reasons are potentially avoidable.
Root causes identifying lack of surgical theatre time were not investigated in this study. Over-booking of operative lists is a potential avoidable root cause [11]. Surgeons may feel optimistic in their estimates, pressured from the long waiting lists or even fear of blame for not working hard enough. No policies were found at JUH to outline the process of operative lists scheduling to avoid overbooking. Van Veen-Berkx and van Dijk [12] have reported that scheduling the anesthesia- and surgeon-controlled time more accurately leads to fewer case cancellations in a university hospital setting. A third component of operative theatre time is the time wasted between scheduled operations [13]. No policies at JUH outline the expected timelines of operative theatre times.
Incomplete preoperative assessment is another reason of priority at JUH. Root causes of this reason were not investigated in this study. These cancellations may be due to the preoperative assessment commencing on the evening preceding surgery, with some of the assessments shifting to the day of surgery [14]. No policies present at JUH to outline the expected timelines for completion of preoperative assessments. A preoperative assessment clinic where patients complete their preoperative assessments days before their surgery is another potential solution. This has been shown to be an effective measure in minimizing cancellation rates [15]; however, this seems difficult to establish at JUH given the available resources and the large number of operations performed per month.
Although guidelines exist for the treatment of elevated blood pressure, there remains a paucity of literature and accepted guidelines for the perioperative evaluation and care of patients with hypertension who undergo noncardiac surgery [16]. Other possible contributing factors for operation cancelation due to high blood pressure include poor blood pressure monitoring preoperatively and inappropriate/inadequate pharmacologic therapy. JUH lacks guidelines on management and monitoring of hypertension in preoperative patients.
Cancellations due to URTI is a complex issue. Informed consent, good clinical judgment and experience are crucial factors in the decision-making process [17]. JUH also lacks guidelines on cancellations of operations due to suspected URTIs.
Based on the previous results, future interventions to reduce operation cancellations need to be directed toward the multifactorial reasons specific for this institution. It has been suggested that patients themselves should select the date of surgery, and receive early notice of their operation day [18]. In addition, most cancellations can be avoided by redesigning work pathways, improving planning and coordination, and performing earlier clinical preassessment of patients [1819].
The significance of this study is that it is the largest and longest series reporting on operation cancellation rates in Jordan. It is also the first to prioritize these reasons according to frequency to direct future improvement measures. There are some limitations, however. First, operation cancellation is a complex and multifactorial process, which subjects this study to bias, especially when assigning a single cause for cancellation when there are several contributing factors or ambiguous causes for cancellation. Future studies can minimize this by relying on a team consensus approach to make the final assessment in ambiguous and multifactorial cases rather than relying on one individual. Another limitation is the documentation bias of the retrospective design.
In conclusion, this study identified the most common reasons for operation cancellation at a single teaching hospital. Future interventions to reduce operation cancellations need to be institution-specific and should take into account the multifactorial dimension of the problem. After identification of the reasons of priority, further focused studies are needed to identify the potential avoidable root causes and to recommend interventions accordingly. Available resources, hospital policies and strategic measures should be directed to eliminate those causes first. Future studies should also look at the outcome of implementation of these policies and strategies on the rate of operation cancellation, quality of care, and resources utilization.


 XML Download
XML Download