

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the advent of high-pressure compressed air in industrial work, the risk of associated pneumatic injuries from its improper use is becoming evident. Among pneumatic injuries, colon injury by accidental insufflation is one of the most serious because an enormous amount of air can be delivered into the rectum in a very short time. It is not well recognized by the public that the pressure of compressed air can penetrate barriers such as clothes and the anal sphincter thereby causing severe colon injury. These injuries usually happen through careless use, but cases resulting from practical jokes have also been reported. The author encountered a case of pneumatic rectal perforation that needed emergency surgical intervention.
CASE REPORT
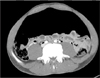
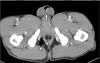
A 40-year-old male factory worker was admitted to the emergency room with severe abdominal pain and distension. Four hours prior, his friend blew out dust from the clothes of the patient with a compressed air gun (Fig. 1) as was usually done in his work place. At this time, his friend placed air nozzle too close to the buttocks of the patient, but the intention of practical joke was denied according to a witness. Immediately, the patient experienced severe abdominal pain and gradual distension of the abdomen. At admission, his blood pressure was 170/104 mmHg, pulse rate was 133 beats/min, respiratory rate was 22 breaths/min, and body temperature was 36.8℃. The patient was pale and clammy. The abdomen was markedly distended with signs of tenderness and rebound tenderness. Large amounts of fresh and clotted blood gushed out on digital rectal examination. On laboratory blood test, white blood cell count was 6.78 × 103/µL, hemoglobin 16.1 g/dL, while the other parameters were not clinically significant. Abdominal X-ray showed large amounts of free peritoneal gas. Computed tomography of the abdomen and pelvis demonstrated large amounts of free gas in the peritoneal cavity, retroperitoneal area, and mediastinum (Fig. 2). Subcutaneous emphysema was seen in the perineal area and around the scrotum (Fig. 3). Percutaneous decompression of the tension pneumoperitoneum was performed by inserting a cannula into the abdomen for relief of pressure. Sigmoidoscopy was attempted after enema for the detection of the perforation site but it did not revealed any significant findings due to the presence of large amounts of fecal material and blood clot in the rectum. Emergency exploratory laparotomy was done under the lithotomy position, which provides a route for intraoperative colonoscopy when necessary. The peritoneum was assessed via a low midline incision. On opening the abdomen, large amounts of air whistled out of the abdominal cavity. Large amounts of gross fecal material and bloody ascites were found. A 4- × 4-cm-sized perforation (Fig. 4), which extended from the retroperitoneal part of rectum to the rectosigmoid junction, was found. Intraoperative endoscopic rectal examination after rectal irrigation was done to evaluate the entire length of the rectum since the presence of perineal air suggested additional rectal injuries; however, there was no other damage. Primary repair of the perforation or anastomosis after bowel resection seemed dangerous under the circumstance of severe fecal contamination. The damaged segment of the bowel was resected with closure of the distal rectal stump and construction of an end sigmoid colostomy (Hartmann procedure). His follow-up period was completed without any complication and he was discharged 8 days after operation. Reversal of the colostomy was done after 8 weeks and the postoperative period was uneventful.
DISCUSSION
Dozens of pneumatic colon injury cases have been reported since the first report by Stone in 1904 [1]. Case analysis often reveals unwise behavior. Those cases not involving misbehavior usually occurred when employees used air hoses to dust off their clothing as in the present case. It is important to realize that this injury can occur without inserting the air hose into the anus. Colorectal injury can occur when the nozzle is merely placed near the anus, even when clothes are worn [23]. It took only 1 to 2 seconds to deliver enough air to cause major damage.
Andrews, using compressed air to distend the intestine of a dog, found that normal intestine required a pressure of 0.49–0.88 kg/cm2 to get ruptured [4]. Burt showed that the average pressure needed to cause a full thickness tear in human gastrointestinal tracts is 0.29 kg/cm2 [5]. In industrial fields, highly compressed air, exerting higher than 10 kg/cm2, is widely used. It is far greater than the pressure needed for intestinal perforation. Highly compressed air is known to form a column that acts like a solid body forcing open the anal sphincter [4]. The funnel shaped anatomy of the buttock facilitates the air to concentrate around the anus and allows the easy delivery of air through the anus. Clothes do not protect the force of compressed air as shown by the fact that almost all cases were fully dressed.
The cecum, having the largest diameter in colon, is the most susceptible site for iatrogenic barotrauma and is explained by the law of Laplace where the tension in the wall is proportional to the radius of the lumen [6]. Meanwhile, most compressed air related injuries occur in the rectosigmoid region. Pneumatic injury is relatively rare in the anal canal and distal rectum since these parts are well supported by external structures and are anatomically straight. The rectosigmoid region, having many flexures, is the first part of the colon to be struck by a column of air. Therefore, most reported injuries occur in the rectosigmoid junction, sigmoid colon, and sigmoid-descending junction [237]. However, colon perforation can occur in other sites including the transverse and ascending colon [89].
When a lage amount of gas is introduced into the peritoneal cavity, respiratory distress occurs due to increased intraabdominal pressure. The elemination of air using a large bore needle is a simple and effective method for relieving pneumoperitoneum tension and respiratory distress as shown in the present case.
After recovery from the initial shock, peritonitis due to fecal contamination should be checked for and treated immediately. The diagnosis is not difficult if the patient has a history of abdominal pain and distension after exposure to compressed air. On radiologic examination, a distended colon filled with air or a large amount of free air in the peritoneal cavity is observed. Colon perforation itself should be treated according to the general principles of treatment for colon perforation. For the perforation of the colon, various types of treatment are possible from conservative management at colonoscopic damage to aggressive surgical treatment. Surgical exploration should garner greater consideration in cases of compressed air induced colon injury with pneumoperitoneum since it accompanies fecal contamination, and preoperative evaluation of the extent of damage is difficult. Conservative managemet would also be possible in mild cases of peritonitis. At the time of laparotomy, primary repair, segmental resection, with or without colostomy, can be performed depending on the extend of contamination.
Primary repair or anastomosis after resection was not appropriate for the present case as the fecal contamination was severe and the bowel was edematous. It should be remembered that a second operation might be necessary in cases of delayed colon perforation [9]. The prognosis has generally been favorable in recent years, although early collective reviews reported grave results [10].
The careless use of compressed air results in catastrophic results as shown in this case. Therefore, workers handling compressed air should be made aware of the hazards before allowing them access. The potential dangers should be prominently displayed in writing in places where it is being used to minimize such accidents in the future.


 XML Download
XML Download