

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Small bowel obstruction (SBO) describes interruption of normal flow of intestinal contents in the small bowel, and is a common complication after abdominal surgery. It may result in unplanned hospitalization, additional costs, and even surgical intervention [12]. Although postoperative adhesions are mainly responsible for SBO, causes other than a history of abdominal surgery, including malignancies or hernias, should be considered. An undescended testis can easily be detected and surgically treated in a younger patient, and is not usually suspected as a cause of SBO in an adult, because of its rarity [34]. Herein, we report a case of SBO caused by cryptorchidism in an adult with no history of abdominal surgery.
CASE REPORT
A 67-year-old man presented to the Emergency Department with nausea, abdominal pain, and distention for 1 day. He was married and had 2 children, and denied any history of abdominal surgery. However, he had a history of several hospitalizations due to small bowel ileus, dyspepsia, and gastroenteritis. Physical examination revealed a distended abdomen with hypoactive bowel sounds. The laboratory data were within normal limits, except for leukocytosis (11,990/µL). Abdominal radiography showed diffuse dilatation of small bowel loops (Fig. 1), and CT showed mildly decreased enhancement of some ileal loops in the left lower abdomen, with ascites in the subphrenic space and paracolic gutters.
The patient was initially treated with a nasogastric tube, hydration, and antibiotics. However, abdominal pain and distention worsened after 1 day, and we performed emergency surgery. On laparoscopic exploration, distended small bowel loops were noted; the terminal ileum was not retracted because of tension of uncertain origin. Dilated small bowel hindered further laparoscopic exploration, so we converted to open laparotomy. After conversion, we found that the terminal ileum was rotated 180° clockwise, and an adherent left testis was noted at 30 cm proximal from the ileocecal valve (Fig. 2). From that point, the proximal small bowel was dilated, and the distal small bowel was collapsed. Bowel ischemia or perforation was not observed. The left testicular vessels and vas deferens fixed the terminal ileum, acting like “adhesive bands,” were ligated. Left orchiectomy was performed, and small bowel continuity was preserved. The final pathologic report was atrophic testis (5 cm × 4 cm × 2.5 cm) without malignancy (Figs. 3, 4). The patient made an uneventful recovery and was discharged 10 days after surgery.
DISCUSSION
Cryptorchidism is usually diagnosed and treated in early life, with an incidence of 1%–4% at the age of 1 [45]. It requires surgery because of the possibility of trauma, torsion, infertility, and malignancy [356]. However, cryptorchidism can be diagnosed in adults, and the treatment of choice is orchiectomy, if fertility is not a concern. The patient in our report had never sought care for urinary, sexual, or fertility problems. Hence, the diagnosis was delayed until symptoms developed.
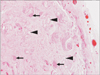
The pathologic report revealed features of atrophic testis, including scattered nests of Leydig cells hyperplasia with hyalinization of seminiferous tubules without any spermatid (Fig. 4). Malignant cells were not found in the specimen, unlike the previous reports that suggested a possibility of malignant potential of undescended testis [34].
Because postoperative adhesions are the most common cause of SBO, abdominal surgical history should be considered first. If the patient has undergone abdominal surgery, the treated site or organ could provide clues to the location of adhesions or a transitional zone. However, if the patient denies prior abdominal surgery, other causes should be considered, such as malignancies, hernias, and even strictures of the small bowel due to inflammatory bowel disease, including Crohn disease.
Although cryptorchidism is not a common cause of SBO, this patient presented with symptoms caused by adhesion between an undescended, intra-abdominal testis and the terminal ileum. There are many reports about the causes, complications, and treatment of cryptorchidism, as well as the potential for infertility or malignancy. However, few reports have investigated the correlation between cryptorchidism and an ileus or SBO in children [78]. To the best of our knowledge, this is the first report of SBO caused by unilateral cryptorchidism in an adult.
In conclusion, among the causes of SBO in male patients without a history of abdominal surgery, surgeons should also consider cryptorchidism as part of a careful history and physical examination.



 XML Download
XML Download