

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Type 2 diabetes mellitus (T2DM) is a chronic progressive disease that is increasing in incidence globally. According to the 2012 Report on Korean Diabetes Research, 10.1% of adults over 30 years of age were diagnosed with diabetes in 2010 [1]. The International Diabetes Federation estimated that the number of people with diabetes in 2003 was 194 million and the projected number of people with the condition in 2025 will be 334 million [2]. T2DM is one of the major comorbid conditions that is related to obesity, and bariatric surgery is strongly recommended for morbidly obese T2DM patients. In the Asian population, the incidence of T2DM is much higher than in Western patients with similar body mass index (BMI) [3]. In Korea, more and more bariatric surgeries are performed with the increased interest in obesity related health care [45].
Although the degree of postoperative weight loss appears to be the major factor of improvement in glucose control following bariatric surgery, diabetic control starts before the patient achieves a sufficient level of weight loss, particularly following Roux-en-Y gastric bypass or biliopancreatic diversion [6]. These early antidiabetic effects are explained by increased levels of incretin hormones, such as glucagon-like peptide-1 or gastric inhibitory polypeptide [7]. Bypassing the duodenum and proximal jejunum is believed to decrease the anti-incretin hormone level. This hypothesis is called the foregut theory, which has been proposed for successful diabetic control. Rubino et al. [8] suggested duodenal-jejunal bypass as a metabolic surgery in a nonobese T2DM animal model. Thereafter duodenal-jejunal bypass was tested in several studies with satisfactory results [1910]. However, these studies only reported short-term results and were designed as single-arm studies. Therefore, we evaluated the outcomes after laparoscopic duodeno-jejunal bypass (LDJB) versus laparoscopic Roux-en-Y gastric bypass (LRYGB) in a 3-year follow-up.
METHODS
During the period from January 2008 to December 2009, LDJB and LRYGB were performed in 17 and 51 patients with T2DM, respectively. LDJB was conducted for patients with BMI less than 30 after approval of institutional review board. LRYGB was indicated for patients whose BMI ≥ 30 kg/m2 with T2DM. In this study, we only included the patients whose follow-up laboratory data were all available for 3 years. After excluding patients who were not available to obtain additional postoperative laboratory data, 8 LDJB and 20 LRYGB patients were included in this study. Retrospective chart review was conducted for these patients.
Surgical procedure for LRYGB
The patient was placed in a supine position and trocar placement was done. The first 12-mm optical trocar was inserted at the left side with using a 0° videoscope. Pneumoperitoneum was created with a pressure of 15 mmHg. After introduction of a 30° scope, rest trocars were inserted under direct visual control. A liver retractor was introduced through the subxiphoid. The jejunum was divided at 40–50 cm distal to the ligament of Treitz. A stapled end-to-side jejunostomy anastomosis was performed with a 100- to 120-cm Roux limb. The remaining enteroenterostomy defect was closed with a continuous suture. All mesentery defects were closed with nonabsorbable sutures. The dissection began directly on the lesser curvature of the stomach, and a 15- to 20-mL gastric pouch was created using multiple laparoscopic linear staple.
The Roux limb was delivered via an antecolic antegastric route. Gastrojejunostomy was performed with an endoscopic linear staple with 2.5-cm length of stoma. Posterior and anterior portions of gastrojejunostomy site were all reinforced with non-absorbable suture material.
Surgical procedure of LDJB
All LDJBs were performed using a laparoscopic approach with similar trocar placement with LRYGB. The length of the biliopancreatic limb was 70 cm from the ligament of Treitz and the length of the Roux limb was 100 cm. Thus, ingested food was able to bypass the duodenum and proximal jejunum. The procedure began by elevating the greater omentum into the upper abdomen. First, the jejunum that was 70 cm distal to the ligament of Treitz was identified and divided using laparoscopic linear staple. The mesentery was divided in a similar fashion. From the point of transection, 100 cm of the small bowel was preserved and an enterotomy was created 170 cm from the ligament of Treitz (Fig. 1). The Endo-GIA stapler (Covidien, Mansfield, MA, USA) was used to create a jejunojejunostomy. The enterotomy site was closed via a hand-sewn anastomosis. Then, the small bowel mesenteric defect was closed with a running nonabsorbable suture. The duodenum portion that was 3–4 cm distal to the pyloric ring was dissected with an ultrasonic scalpel. A silastic tube was used to secure the dissection of the posterior duodenum. Then duodenum was transected with linear staple. Duodenojejunostomy was made using stapling methods
Clinical assessment and Follow-up
Baseline characteristics of patients in both groups, including sex, age, BMI, DM duration, preoperative glycosylated hemoglobin (HbA1c), and C-peptide levels, were evaluated. During the follow-up period, serial changes in body weight, BMI, HbA1c were evaluated every 3 months postoperatively for 1 year and then annually thereafter. We assessed the effectiveness of diabetic control postoperatively over the period of 3 years by comparing HbA1c levels and type of antidiabetic treatment. We defined response to diabetic control using the following definition.
Definition of DM control
Remission – maintaining HbA1c ≤ 6 .5 w ithout o ral hypoglycemic agent (OHA) or insulin.
Improve – decreasing dose of medication or converting OHA from insulin.
No interval change – no definite change in dose of medication and HbA1c.
Aggravation – increasing dose of medication or converting to insulin from OHA.
RESULTS
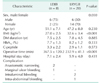
In total, 8 LDJB and 20 LRYGB patients were analyzed. More male patients in the LDJB group (LDJB 75% vs. LRYGB 30%, P = 0.030). Baseline BMI in the LRYGB group was significantly higher than in the LDJB group (LDJB 27.0 ± 2.5 vs. LRYGB 32.6 ± 3.4, P < 0.001). Age, DM duration, baseline HbA1c (LDJB 7.7 ± 1.3 vs. LRYGB 8.2 ± 1.2, P = 0.333), and C-peptide level (LDJB 3.3 ± 2.2 vs. LRYGB 2.9 ± 1.1, P = 0.573) were similar (Table 1).
Based upon the results of surgery, a longer operation time was needed in the LDJB group (LDJB 367.5 ± 120.2 vs. LRYGB 232.9 ± 41.1, P < 0.001). Based upon postoperative complications, 2 cases of anastomotic narrowing and 1 case of marginal ulcer bleeding were observed in the LDJB group. Two cases of intraluminal bleeding and 1 case of intra-abdominal bleeding were observed in the LRYGB group (Table 1).
Based upon changes in body weight, continuous weight loss was maintained during the first year following operation in the LRYGB group (Fig. 2A). Meanwhile, the mean weight increased from the postoperative third month in the LDJB group (Fig. 2B). Compared to BMI difference from the baseline, there were continuous significant decreases in BMI from postoperative 1 month to third year in LRYGB compared with LDJB (Fig. 2C). The mean HbA1c difference from the baseline level decreased considerably in the LRYGB group and showed a significant difference at 6 months and 2 years following operation compared with LDJB (Fig. 2D).
At the 3-year follow-up period, the DM remission rate was observed for 40% of cases in the LRYGB group and no patient showed DM remission in the LDJB group. In the LRYGB group, all patients showed an improvement in DM control. In LDJB group, only 37.5% of patients showed an improvement in DM control. The others showed no interval change or aggravation of DM status (Table 2).
DISCUSSION
In present study, LDJB failed to show a long-term effect for glucose control in nonmorbidly obese patients. Roux-en-Y gastric bypass is one of the most commonly performed bariatric surgeries and it has 2 surgical alterations. One is a restriction of gastric volume and the other is diversion of ingested nutrients away from the proximal small intestine. While LRYGB is performed frequently in morbidly obese patients, the factors that contribute to early diabetic control are still not clearly established. Rubino and Marescaux [11] first performed animal studies to confirm the effect of bypassing the proximal small intestine and demonstrated that experimentally performed duodeno-jejunal exclusion showed a positive effect on glucose control in nonobese T2DM models. This group attempted to determine the mechanism of glucose control in the absence of significant weight loss under the two hypotheses, which included “hindgut theory” and “foregut theory” [8]. Foregut theory was regarded as the favorable theory, which included suppression of undetermined anti-incretic secretion for diabetic control in nonobese rats. This concept of duodeno-jejunal bypass was adopted for use with endoscopic procedures, such as endoscopic duodeno-jejunal bypass linear. This procedure showed considerable effect in weight loss and metabolic effect [1213]. Another study suggested that specific entero-endocrine cell populations may have a critical role in normalizing glucose homeostasis [14].
Owing to these findings of metabolic effects in nonobese rat, several human studies were performed. The procedure was first performed in T2DM patients with a BMI less than 35 kg/m2, after approval from Yeouido St. Mary's Hospital Institutional Review Board (approval number: SC14RISI0164) and obtaining informed consent from patients [9]. In that report, total seven patients were included and underwent 1 year of follow-up. Some patients showed an improvement in diabetic control with less doses of insulin. Preliminary clinical data performed in our institute also showed favorable results at 1 year of follow up [10]. In another Korean study, Heo et al. [1] reported the results of DJB in T2DM patients with a normal BMI range. In this report, 13.3% of patients exhibited remission of T2DM and 26.7% of patients exhibited an improvement in glucose control at the postoperative 12-month period. In spite of these short-term result of DJB procedure, there are scarce reports regarding the results at more than 1 year after LDJB. To confirm the real effect of LDJB, long-term data must be observed. In the present study, we included patients whose follow up was completed for 3 years. For effective comparison, we used T2DM patients who had undergone LRYGB as a control group because LRYGB is an established bariatric procedure for metabolic effect. Although there are significant discrepancies in baseline weight between the 2 groups, there were no differences regarding their diabetic status.
According to the American Society of Metabolic and Bariatric Surgery consensus meeting, currently accepted bariatric procedures include LRYGB, sleeve gastrectomy, gastric band, and duodenal switch. LDJB is not a generally accepted procedure and it is performed only in clinical trials with IRB approval [15].
In the present study, we observed early weight change and diabetic improvements until postoperative 1 year. Although LDJB did not comprise restrictive surgery, early weight change was achieved along with decreased HbA1c and glucose control. However, unlike after LRYGB, weight was regained and glucose control was deteriorated. It is not sure what mechanism evoked the early weight change and glucose control, but decreased calorie intake or anti-incretin effect may be contributing factors. Nevertheless, it is clear that all the early changes are rectified within 1 year.
The final goal of LDJB was to find a way of achieving glucose control in T2DM patients with a normal BMI. According to the present study, the action of foregut theory cannot cover glucose control in T2DM patients with normal BMI without other additional procedures.
Laparoscopic biliopancreatic diversion/duodenal switch (BPD/DS) is 1 type of traditional bariatric operations. Recently, modified procedure sleeve plus DJB procedures were introduced and showed excellent results regarding glucose control [1617]. This new procedure may be a modified form of BPD/DS with a difference in the length of the bypassed jejunum. A recent study comparing sleeve gastrectomy and sleeve-plus-DJB showed more effective results of sleeve-plus-DJB than did the sleeve-only procedure regarding T2DM control [18]. This finding demonstrates that the bypassing factor has some effect. However, we cannot determine the what precise factor causes the difference. Nevertheless, It is true that additional restrictive procedures should be considered.
It is important to consider the correlation of obesity and T2DM. In the present study, LDJB patients are not morbidly obese patients, who are otherwise excluded from bariatric surgery. Mechanism of T2DM development might be different between the 2 groups.
In this study, there were several limitations. First, the present study is retrospective in nature and many patients were lost to follow up. The other limitation is that baseline indications and characteristics were different between the 2 groups. However, although the LRYGB group included heavier and poorly controlled diabetes patients, postoperative 3-year data showed similar status of BMI and improved HbA1c levels in the LRYGB group. These results demonstrate sustained weight loss effect and glucose control in the LRYGB group as well as nondurable glucose control in the LDJB group.
In conclusion, LDJB is not an effective method for controlling T2DM compared with LRYGB. Foregut theory may not be the main mechanism of diabetic control during bariatric surgery.



 XML Download
XML Download