

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A pheochromocytoma is an uncommon catecholamine-secreting tumor from chromaffin cell of the adrenal gland. It affects approximately 0.1%–0.6% of hypertensive individuals [1]. Rupture of pheochromocytoma is an extremely rare, emergent, and lethal clinical condition. A total of 50 cases of pheochromocytoma have been reported worldwide [2]. Only 2 cases have been reported in Korea. The mortality rate of ruptured pheochromocytoma is 50% in Korea [34]. It is approximately 31% worldwide [2]. The causes of mortality include bleeding, heart failure and multiorgan dysfunction from excessive release of catecholamine, postoperative severe hypotension, and pulmonary edema [2]. Correct diagnosis and elective surgery after controlling blood pressure are the most important prognostic factors. We report a case of spontaneous rupture of the left adrenal pheochomocytoma in a 44-year-old male patient presenting abrupt onset of left flank pain with uncontrolled blood pressure who was successfully treated by emergency operation. We also propose the correct treatment for ruptured pheochromocytoma through literature review.
CASE REPORT
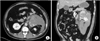
A 44-year-old male patient visited our Emergency Department and presented with abrupt onset of left flank pain, headache, cold sweeting, and palpitation during the past 4 hours. He had a past medical history of hypertension. His blood pressure was 190/140 mmHg with purse rate of 130 beats/min on arrival. His respiration rate and body temperature were normal. He was restless and his blood pressure was increased from 90/40 to 200/150 mmHg by changing position. A complete blood count revealed elevated levels of WBC count (20.50 × 109/L), hemoglobin (17.1 g/dL), and platelet (285,000/mL). Blood chemistry showed elevated serum osmolarity (306 mOsm/kg) and serum glucose level (263 mg/dL). Abdominal CT was performed at the Emergency Department. It showed a heterogeneous mass at size of 8.1 cm × 5.6 cm with rupture on the left retroperitoneal space and hematoma with active bleeding around the mass (Fig. 1). His symptom of abdominal pain was aggravated. Follow-up laboratory analysis revealed elevated WBC count (30.15 × 109/L) but decreased hemoglobin level (15.7 g/dL) 2 hours after admission. Emergency exploratory laparotomy was performed because persistent bleeding and infection were suspected. During exploration, ruptured left retroperitoneal mass with hematoma and bleeding anterosuperior to the left kidney were noted. During anesthesia, patient's blood pressure was elevated up to 210/130 mmHg. It was dropped after the removal of tumor and hemostasis. Blood pressure was stable after fluid challenge and dopamine administration. He was transferred to the general ward on the 4th postoperative day. He was discharged on the 9th postoperative day without complication. Pathologic exam revealed 5 × 3 × 2-cm-sized adrenal pheochromocytoma with rupture. Abdominal CT, chest CT, and whole body PET-CT were performed to rule out malignant pheochromocytoma and distant metastasis at 3 months after surgery and revealed no significant evidence of metastasis or recurrence. In addition, 24-hour urinary vanillymandelic acid (VMA) and metanephrine were checked. They had normal values (VMA, 3.5 mg/day; metanephrine, 0.407 mg/day). The patient recovered in good health with normal blood pressure. He has been followed-up every year.
DISCUSSION
Ruptured adrenal pheochromocytoma is extremely rare. It can be lethal. Up to date, 2 such cases have been reported in Korea [34]. Since its first report by Cahill in 1944, a total of 50 cases of pheochromocytoma (38 cases of ruptured and 12 cases of hemorrhagic) have been reported from the 1950s to 2000s in worldwide. Its mortality rate is 50% in Korea and 34% worldwide [2345]. Major causes of perioperative mortality are hypovolemia from hemorrhage, respiratory disorder from pulmonary edema, and heart failure from cathecholamine cardiomyopathy [2]. The cause and mechanism of rupture of pheochromocytoma remain unclear. However, rapid growth of tumor and intratumoral hemorrhage may increase the pressure to the capsule and cause rupture. After the rupture of pheochromocytoma, massive cathecholamine is released into circulation, leading to hypertensive crisis, severe headache, abdominal pain, nausea, vomiting, ileus, paler skin, sweating, and elevation of serum creatinine [6]. Adequate diagnosis of ruptured pheochromocytoma is difficult before operation. Kobayashi et al. [2] have reported that the preoperatively correct diagnosis rate is only 30.2%. Its difficult diagnosis may result from its extremely rare incidence. In addition, the measurement of cathecholamine at either serum or urine level is impossible under emergency situation.
The only treatment of ruptured pheochomocytoma is surgical resection either through emergency or elective operation. The most important prognostic factor is good blood pressure control using α-adrenergic blockade and fluid replacement preoperatively. Based on literature review, emergency surgery without proper blood pressure control and incorrect preoperative diagnosis are strongly associated with poor prognosis [2]. Total of 2 cases in Korea was performed emergency operation without blood pressure control and 1 case was died because of pulmonary edema with heart failure after operation [34]. However, there is no mortality in patients who undergo elective surgery after medical therapy [2]. Preoperative management for hypertensive crisis is using α-blockers such as phenoxybenzamine because they can block adrenoreceptor noncompetitively. Propranolol is also available for cardiac arrhythmia [7]. Angiographic intervention for hemostasis has also been successfully applied in patients with rupture and active bleeding. Habib et al. [8] have reported 3 cases of ruptured pheochromocytoma with bleeding and rupture successfully treated by elective resection after controlling blood pressure by transcatheter arterial embolization (TAE). Each gland is supplied by the superior, middle, and inferior suprarenal arteries, which arise from the inferior phrenic artery, abdominal aorta and renal artery respectively. A TAE using coli was performed on these blood vessels using microcatheters. Total body water control can also be achieved using α-adrenergic blocker and fluid infusion therapy or after stabilization by TAE. They performed elective adrenalectomy after 1 month. The preoperatively application of TAE allows for hemostasis and can be performed easily and without complication such as hypovolemic shock [8].
Although our patient is alive through emergency exploration and resection of pheochromocytoma without good management of blood pressure, proper treatment of ruptured pheochrmocytoma is not emergency operation, but elective operation after controlling blood pressure either with medical method or interventional method for active bleeding. Furthermore, correct diagnosis was also important for preoperatively proper management.
 XML Download
XML Download