

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
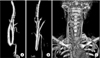
Takayasu arteritis (TA) is a nonspecific granulomatous inflammatory arteriopathy of unknown cause that results in arterial occlusion and stenosis due to inflammatory fibrosis, calcification, and hematoma. TA also less commonly causes aneurysmal degeneration of large and medium-sized elastic arteries (Fig. 1) [1]. The disease was first described in 1908 by Takayasu [2], a Japanese ophthalmologist, in a young female patient with retinal neovascularization and an absent radial pulse. Subsequent descriptions of the disease have emphasized the ‘pulseless’ syndrome, with involvement of the brachiocephalic arteries. Its incidence is low, being reported in 1/3,000 autopsies in Japan and as low as 2.6 cases per one million in the United States [34]. The female-to-male ratio was reported as 8–10:1 [5].
The clinical signs depend on the type of organ involvement. Patients present with claudication if the lower abdominal aorta is involved, hypertension if the renal arteries are involved, angina and myocardial infarction symptoms if the coronary arteries are involved, and cerebrovascular symptoms if the cerebrovascular vessels are involved.
In contrast to patients with atherosclerosis, TA patients are young but have severe organ dysfunction according to the particular organ artery involvement, and these patients typically undergo extensive medical evaluation prior to surgery. The surgical procedure has historically consisted of a bypass procedure to vessels normal on angiography proximal and distal to the occlusive or stenotic lesion [6].
In particular, severe cerebrovascular ischemia caused by occlusion of the common carotid arteries results in complications such as intracranial hemorrhage (ICH) or intracranial infarction which can manifest as paresis, syncope, dizziness, dysarthria, visual disturbances, uncontrolled headache, hypertension, and other symptoms [78910]. Thus, severe cerebrovascular ischemia due to TA is regarded as an indication for endovascular intervention or bypass surgery [11]. This study evaluated the safety, effectiveness, and postoperative course of bypass surgery in patients who received bypass surgery.
METHODS
Patients
A retrospective analysis was done at a single center, Samsung Medical Center, from March 2002 to April 2015. In this study, 19 patients were identified who received aorto-carotid bypass surgery due to TA with severe cerebrovascular ischemic symptoms including: amaurosis fugax, transient ischemic attack, syncope, difficulty in raising the head due to vertigo, headache, neck pain, nausea, numbness, weakness, dysarthria, paresthesia, disorientation, confusion, hallucination, seizures, and other symptoms [1213]. They were found to have occlusion of the common carotid arteries or the aortic arch vessels.
Study design
The diagnosis of TA was made when at least 3 of the 6 criteria outlined by the American College of Rheumatology were met [14]. For evaluation of the diseased arterial system, conventional angiography, CT angiography, or MR angiography was performed [151617]. Unilateral common carotid artery involvement was identified in 11 patients and bilateral common carotid artery involvement was identified in the remaining 8 patients.
Surgery was done after normalization of ESR and CRP level by using steroids and immunosuppressants like prednisolone or methylprednisolone. All patients were medicated with anticoagulant agents or antiplatelet agents like aspirin, clopidogrel, cilostazol, nadroparine, warfarin, or rosuvastatin during the preoperative and postoperative periods.
The interval from diagnosis to operation, operation type, and graft type was also investigated. The cases were also reviewed concerning any complications, especially postoperative critical complications such as ICH and infarction by identifying the symptoms of patients and radiologic examination like brain CT or brain MRI.
In addition, postoperative blood pressure (BP) was investigated in all patients and patients were categorized into an uncontrolled and a controlled BP group. BP was measured at the brachial artery in the upper arm of the patients by noninvasive methods like BP cuff and patient monitoring was performed every hour at intensive care unit with periodic BP checks per 6- to 8-hour intervals at ward. The criteria for an uncontrolled BP in the present study was defined as a systolic BP over 180 mmHg at least one time despite administration of antihypertensive medication like calcium channel blocker, beta blocker, alpha blocker, or diuresis within 1 week after surgery. The relation between BP control and ICH was analyzed by Fisher exact test.
This retrospective data collection and analysis were approved by the Institutional Review Board of the Samsung Medical Center and were carried out in accordance with approved guidelines (approval number: 2016-03-069).
Aorto-uni-carotid bypass
This operation was performed in the 11 patients found to have unilateral carotid involvement. An oblique skin incision along the anterior border of the right sternocleidomastoid muscle and a median sternotomy were made. After intravenous heparin injection, the ascending aorta was partially clamped and the aorto-uni-carotid bypass was constructed with externally supported expanded polytetrafluoroethylene (e-PTFE) or a saphenous vein graft (Fig. 2). The graft was positioned along the course of the original carotid artery.
Statistical analysis
The distribution and proportion of various categorized lists were analyzed by descriptive statistics. The comparison of distribution between subgroups according to interval was analyzed by Mann-Whitney test. The relation between BP control and ICH was analyzed by Fisher test. All reported P-values were 2-sided and the significance level was set to 0.05. Statistical analyses were carried out with SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
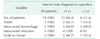
All patients were female and the range of their age was 15 to 66 years with a mean age of 40.6 ± 15.3 years (mean follow-up duration, 61.0 ± 42.4 months; range, 1–138 months). The time interval from diagnosis of TA to operation was also investigated. Thirteen patients (68.4%) had intervals less than 3 years between diagnosis and operation with a mean interval time of about 1 year (mean, 13 months; median, 10 months). Eight of those patients (42.1%) had an interval less than 1 year. Six patients (31.6%) had intervals more than 3 years with a mean interval between diagnosis and operation of about 18 years (mean, 222 months; median, 289 months) (Table 1, Fig. 5). All results of the analyses of interval distribution between (≤1 year vs. >1 year) or (≤2 years vs. >2 years) or (≤3 years vs. >3 years) showed the same P-value of 0.000. Inquiring on the relation between the interval and complications, expiry, ICH, intracranial infarction, graft occlusion more frequently occurred in the group below 3 years than over 3 years of intervals (Table 2).
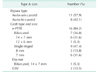
Eleven patients (57.9%) with unilateral common carotid artery involvement underwent aorto-uni-carotid bypass and 8 patients (42.1%) with bilateral common carotid artery involvement underwent aorto-bi-carotid bypass. Sixteen patients (84.2%) were interposed with an e-PTFE graft, 1 patient (5.3%) was interposed with a Dacron graft, and 2 patients (10.5%) were interposed with a saphenous vein graft. Among the e-PTFE graft cases, there were 7 cases (36.8%) for which a bifurcated e-PTFE graft was used, and 9 cases (47.4%) for which a ringed single limb e-PTFE graft was used. Of e-PTFE bifurcated graft cases, 6 cases (31.6%) were 14 mm × 7 mm in size and 1 case (5.3%) was 12 mm × 6 mm in size. Of e-PTFE single ringed graft cases, 3 cases (15.8%) were 8 mm in size and 6 cases (31.6%) were 7 mm in size. One case (5.3%) was applied by a 14 × 7-mm size bifurcated type of Dacron graft (Table 3). As shown in Table 4, the graft type in patients who expired, ICH, intracranial infarction and graft occlusion was analyzed (Table 5).
Five patients (26.3%) suffered an ICH within 8 days after bypass surgery. Of these cases, 2 patients (10.5%) expired on 26 days, 7 years after surgery and 3 patients (15.8%) with symptoms spontaneously resolved. Four patients (21.1%) suffered an intracranial infarction at diverse times (2 weeks, 1 month, 4 months, 9 years) after bypass surgery. Of these patients, 1 patient (5.3%) expired 9 years after bypass surgery and 3 patients (15.8%) with symptoms spontaneously resolved. Of note, although 2 patients (10.5%) suffered both an ICH and an intracranial infarction, both survived (Table 5, Fig. 6).
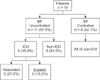
There were 11 patients (57.9%) in the uncontrolled BP group and 8 patients (42.1%) in the controlled BP group. In the uncontrolled BP group, 5 of 11 patients (45.5%) suffered an ICH and of these, 2 of 11 patients (18.2%) expired and 3 of 11 patients (27.3%) recovered spontaneously. In the controlled BP group, no patient suffered ICH and 1 patient (5.3%) expired due to an intracranial infarction (Fig. 7). The statistical result of relationship between BP control and ICH showed a P-value of 0.045.
The cerebrovascular ischemic symptoms resolved in all of the surviving patients. There were no anastomosis site complications such as aneurysm or stricture postoperatively. Firstly, as mentioned before, there were 3 expiries (15.8%), 5 ICH (26.3%), and 4 intracranial infarction cases (21.1%). In addition, there were 3 graft occlusion cases (15.8%), 2 (10.5%) of which tolerated the complication, and 1 patient (5.3%) who suffered intracranial infarction and finally expired. Hyperperfusion syndrome occurred in 4 patients (21.1%) within 2 months after surgery. Symptoms of hyperperfusion syndrome include seizure, cyanosis, hallucination, and headache due to brain edema. One patient (5.3%) developed seizures, cyanosis, and pulseless state with return of spontaneous circulation after cardiopulmonary resuscitation. The other patients improved with symptoms relieved by medication such as anticonvulsants or antihypertensive agents. Hypertensive encephalopathy presents with a number of different symptoms including altered mentation, urination, spit and other symptoms. One patient (5.3%) suffered this complication 2 months after surgery and symptoms were controlled by the anticonvulsants.
There were also cardiovascular complications. Myocardial infarction occurred in 1 case (5.3%) on postoperative day 1 and was improved by critical care. Atrial fibrillation occurred in 2 patients (10.5%) and was controlled by antiarrhythmic agents. A pericardial effusion developed in 1 case (5.3%) and was improved by pericardiocentesis. There was superior femoral artery (SFA) occlusion at 11 months after surgery (Table 5).
DISCUSSION
TA is an idiopathic, chronic inflammatory disease involving the aorta and its main branches. It induces inflammatory, fibrotic changes of the artery wall, and eventually leads to stenosis or occlusion of the artery [1]. It is also associated with arterial calcification and hematoma formation.
The pathologic findings inform the arterial wall changes such as intima hyperplasia, media infiltration, and adventitial fibrosis. These changes are related to the activity of lymphocytes, plasma cells, and giant cells [91819]. The pathologic findings of the patients described here included granulomatous inflammatory, diffuse productive inflammatory, and fibrotic changes of the artery (Fig. 1) [13].
In general, the first choice for management of TA is inflammation suppression using steroids and immunosuppressive agents. As supportive management of TA, using antiplatelet and anticoagulant agents reduces the risk of atherosclerosis and ischemic events [202122]. Uncontrolled TA despite the use of these medications should be treated by surgery or endovascular intervention [202123]. In the same manner, most patients in this study were medicated with steroids or immunosuppressive and anticoagulant or antiplatelet agents. However, all the patients included in this study had poorly controlled disease despite optimal medical management, so they had no choice but to receive surgery.
Consistent with the disease specific epidemiologic features, all patients were female with a mean age of 40 years, relatively young. We investigated if there was any relationship between the interval from diagnosis to operation and the prognosis of the patients. The results of this study showed no significant relationship but showed some trends between these factors. Of note, the interval between diagnosis and the need for operation of most patients (13, 68.4%) was within 3 years, with more than half of these patients (8, 42.1%) requiring operation within 1 year from diagnosis (Table 1, Fig. 5). The distributions of intervals between (≤3 years vs. >3 years) and between (≤1 year vs. >1 year) were significantly different (P < 0.001). This may indicate that most patients who underwent surgery had suffered severe cerebrovascular symptoms within a relatively short period of time after diagnosis.
Also, the other patients with intervals longer than 3 years were relatively small in number (6, 31.6%) and most of them were distributed over 10 years (median, 289 months; interquartile range, 185.5 months). It may suggest that the pace of disease progression and risk of requiring surgical management considerably decrease after 3 years from diagnosis. From a different point of view, it may suggest that the interval group of over 3 years originally had disease specific features more easily controlled by medical management, thereby having a longer interval from diagnosis to operation. In other words, these trends suggest that most patients who underwent surgery had fast disease progression, within 3 years after diagnosis, and it can be related that the interval group below 3 years may be more likely to suffer critical complications after surgery (Table 2). Therefore, taken together, both medical management and close observation within 3 years after diagnosis of TA may be important for prognosticating therapeutic responses and for determining operative timing in TA patients. In order to provide greater clarity, further investigation with a much larger number of cases and longer follow-up periods is required.
There did not appear to be any association between graft type or size and the development of specific complications like expiry, intracranial complications, and graft occlusion (Table 4).
All patients who developed an ICH were in the uncontrolled BP group and there were no ICH patients in the controlled BP group. The statistical results of the relationship between BP control and ICH were significant (P = 0.045). This strongly suggests that BP control is one of the most important factors for decreasing the postoperative risk of an ICH (Fig. 7) [24].
There were 3 patients (15.8%) who expired, with 2 (10.5%) dying due to an ICH and 1 (5.3%) whose death was attributed to an intracranial infarction. This suggests that intracranial complications are significantly associated with an increased mortality risk. All ICH cases occurred within 8 days postoperatively. In contrast, intracranial infarctions occurred at varied postoperative times (Table 5, Fig. 6).
A number of other complications also occurred. One patient (5.3%) with a graft occlusion progressed to develop an intracranial infarction and finally expired. Hyperperfusion syndrome and hypertensive encephalopathy were also found to be strongly associated with postoperative hypertension. These complications can manifest with many concerning symptoms, but are typically well controlled with careful BP management. TA was originally identified as a vascular disease, thereby increasing cardiovascular complications after surgery. Because TA causes vascular inflammation, fibrosis, and calcification, it can cause stenosis or occlusion of any artery. This was reflected in 1 SFA occlusion case (5.3%) in the current case series (Table 5).
Previous studies by Kieffer et al. [25], including recent studies by Reddy and Robbs [26], and Fields et al. [27], showed a low mortality from bypass surgery in TA patients. In addition, we also have reported five cases of aortic bypass or aortic endarterectomy in TA [6] and 2 cases of abdominal aortic endarterectomy in TA and Leriche's syndrome [28]. These studies confirmed that the surgery was safe and effective in TA [29]. The choice of operative procedure depends on the lesions and the number of arteries involved, the extent of arterial occlusive lesions, and the clinical manifestations [30].
The present study was limited by the small number of cases. Therefore, further studies with a larger population size should be done in the future. Surgical treatment of symptomatic TA was found to be effective and relatively safe in patients with severe cerebrovascular ischemic symptoms.
In conclusion, to sum up, aorto-carotid bypass in TA with cerebrovascular ischemia resulted in improvement of ischemic symptoms after surgery. The major complications after bypass surgery were ICH (26.3%) and intracranial infarction (21.1%). The main cause of cerebral hemorrhage was uncontrolled hypertension after surgery. The interval from diagnosis to operation showed some trends. However, we couldn't find significantly correlated outcomes with the clinical course and development of critical complications. The size and type of graft was not found to be significantly correlated with the development of critical complications.
Aorto-carotid bypass is effective for treating patients of TA with cerebrovascular ischemia. Additionally, we need keep in mind that BP should be strictly managed after bypass surgery to prevent postoperative ICH.








 XML Download
XML Download