

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic suturing can be one of the most challenging skills to master in minimally invasive surgery, and the use of V-Loc (Covidien, New Haven, CT, USA) barbed absorbable suture allows surgeons to perform laparoscopic suturing faster and more easily. However, there are reported complications associated with improper use of V-Loc devices. Here we present the case of a patient with postoperative mechanical small bowel obstruction (SBO) after total laparoscopic distal gastrectomy performed using V-Loc barbed absorbable suture. We then discuss how the barbed suture device acted as the underlying mechanism for the SBO and emphasize the need for careful attention to technique in the use of new suture methods.
CASE REPORT
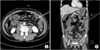
A 64-year-old male developed abdominal pain and distension four days after total laparoscopic distal gastrectomy with Roux-en-Y anastomosis performed for gastric cancer. A CT scan of the abdomen subsequently revealed herniated small bowel between the Roux-limb and the distal bowel requiring immediate surgical intervention (Fig. 1). An elevated C-reactive protein level and leukocytosis were identified on laboratory tests, and an increase in patient's heart rate was monitored.
Laparoscopic abdominal exploration was performed and the cause of the acute herniation and SBO was identified. Intraoperative findings included the discovery that the proximal small bowel had herniated through the space created by V-Loc barbed absorbable suture after jejunojejunostomy (Fig. 2). The herniated portion of the small bowel was pulled out of this space using gentle progressive traction and completely closed laparoscopically. After removal of the surgical clip and the end of the V-Loc, no resection of small bowel was required. The cut suture ends were then embedded into the serosa of the small bowel. The patient was advanced to a regular diet two days after surgery and uneventfully discharged five days postoperatively.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
DISCUSSION
V-Loc unidirectional barbed suture was developed as a device aimed at making laparoscopic suturing easier and more efficient. With its unique barbed design, knot-tying is not needed to anchor these sutures to tissue. Furthermore, another proposed benefit of V-Loc closure is a uniform distribution of force along the suture line, which ensures security of intestinal anastomosis and decreases blood loss [1]. This device may enable surgeons to effectively perform laparoscopic suturing and to shorten the anastomosis time.
The safety and efficacy of barbed suture use for closure of the exit hole after gastroduodenostomy in gastrectomy has been reported [2]. In addition to the benefits of barbed suture use, complications following use of these devices have been reported in the literature for several other surgeries [134]. However, we believe there has not been a reported case presenting a complication of internal herniation and mechanical SBO after laparoscopic gastrectomy using barbed sutures. We report here a case of improper application of a V-Loc device resulting in internal herniation and mechanical SBO after laparoscopic gastrectomy.
Patients undergoing gastrectomy are at a high risk of developing intestinal obstruction. Therefore, intraoperative preventive techniques are recommended [5]. In our case, the bowel obstruction was likely due to the presence of a long and redundant length of wire following the use of barbed suture. To prevent bowel obstruction, the length for the end of the exposed barbed suture during surgery should be kept to a minimum. In summary, surgeons performing laparoscopic gastrectomy using V-Loc suture should consider that improperly deployed barbed suture may induce postoperative mechanical SBO or other complications.
The lesson from this case is that surgeons must be aware of the proper usage of new devices, as well as their potential hazards. This case highlights the need for surgeons to increase their attention to the technical details of new closure materials.

 XML Download
XML Download