

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic cholecystectomy (LC) is the current standard treatment for symptomatic gallstone disease. LC has well-known advantages over open cholecystectomy. However, various surgical complications can occur with LC more than with open cholecystectomy. Bile duct injury is the most common complication in either laparoscopic or open cholecystectomy. Bile duct injury in LC usually occurs when the common bile duct is mistaken for the cystic duct, and is subsequently clipped and divided. However, when anatomical variants or aberrants are present, the right hepatic duct is at increased risk for injury. The low insertion of a right sectoral hepatic duct, either into the common bile duct or at the cystic duct, is an important variant that places this duct at risk of being injured during LC [123]. The conventional treatment for this isolated bile duct injury is a hepaticojejunostomy or hepatectomy. However, there are various difficulties that can arise with repeated operation, though some case reports have demonstrated successful treatment with percutaneous management using sclerosing agents. Here, we present a case of biliary leak from an isolated right posterior sectoral duct (RPSD) after cholecystectomy treated with acetic acid sclerotherapy combined with coil embolization for a fistula tract.
CASE REPORT
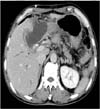
A 67-year-old male patient was admitted for epigastric pain. The patient was diagnosed with acute calculous cholecystitis. Although the patient had a history of abdominal surgery for intestinal perforation, we decided to perform LC. During surgery, we had difficulties with dissection due to the inflamed and fibrotic gallbladder. Bile duct injury occurred during the dissection process, so we had to convert to open surgery. We repaired the injured common bile duct and inserted a T-tube. One day after the operation, a small amount of bilious fluid began to drain via the installed Jackson-Pratt drain at less than 30 mL per day. However, the patient started to run a fever at postoperative day 4, so we performed an abdomen CT scan, which showed fluid collection in the gallbladder bed, extending to the left perihepatic space (Fig. 1). Thereafter, an ultrasound-guided percutaneous drainage (PCD) catheter was inserted to drain the fluid, which was found to be bilious. Although bile drainage occurred through the T-tube, the amount of bilious fluid drained via the PCD catheter was about 400 mL per day, so we performed percutaneous transhepatic biliary drainage (PTBD) on postoperative day 8. PTBD cholangiogram revealed a biliary leak from the RPSD (Fig. 2). Although proper bile drainage occurred through the T-tube and PTBD, the amount of bilious fluid drained from the drain was constant at 100 mL per day without decreasing. Even worse, the pathology of the gallbladder was found to be adenocarcinoma. We recommended re-exploration for complete extended cholecystectomy and right hemihepatectomy for sustained biliary leak from the isolated RPSD, but the patient strongly opposed the surgery, so we decided to perform acetic acid sclerotherapy for isolated RPSD. A short cobra type catheter (A&A MD, Sungnam, Korea) was located in the isolated RPSD. A 7-F balloon occlusion catheter (Boston Scientific, Watertown, MA, USA) was placed in the abscess cavity to avoid leakage of the sclerosing agent into the peritoneal cavity. 9 mL of 50% acetic acid (Duksan Pure Chemicals, Ansan, Korea) was injected into the isolated RPSD (Fig. 3). After 10 minutes, the injected acetic acid was aspirated and then washed out with normal saline. This procedure was repeated in 3 sessions over 8 days. The amount of bile drained through the PCD catheter changed from a decreasing trend to an increasing trend after the third session. Cholangiogram was taken 12 days after sclerotherapy, and showed a fistula tract between the RPSD and the abscess cavity. Using microcoils, the fistula tract and abscess cavity were embolized (Fig. 4). After 2 more sessions, the amount of drained bile decreased to less than 10 mL per day for 3 consecutive days. Follow-up cholangiogram after a total of 5 sessions showed no more leakage, so the PTBD was clamped. For 5 days after PTBD clamping, there was no further bile drainage. The PTBD catheter was removed 25 days after sclerotherapy (postoperative day 39), and the PCD catheter was removed 3 days later (postoperative day 42). During these procedures, the patient complained of abdominal pain and mild fever, but the symptoms were tolerable and disappeared after repeated procedures. Leukocytosis (<15,000/mm3) and elevated serum aminotransferase levels (<150 IU/L) were observed as well. The patient was discharged, and follow-up CT scan 20 days after the completion of sclerotherapy showed markedly decreased subhepatic fluid collection (Fig. 5). A follow-up CT scan 4 months after sclerotherapy showed complete resolution of subhepatic fluid collection but metastatic tumor in the liver. Unfortunately, the patient was lost to follow-up thereafter.
DISCUSSION
LC is the current standard treatment for symptomatic gallstone disease due to its well-known advantages. Bile duct injuries following cholecystectomy can occur during either open or laparoscopic surgery. In spite of the many advantages that have made laparoscopic surgery the standard for the treatment of gallstone diseases, the risk of bile duct injury appears to be increased by this technique [1]. The incidence of bile duct injury as a LC-associated complication is 0.5%–1.4%, and varies in terms of extent and location [2]. Bile duct injury following LC often results from the misidentification of anatomy and anatomic variations within the biliary tree. The most common biliary anomaly is an aberrant insertion of the RPSD into the biliary tree, usually inserting close to the cystic duct [345]. The low insertion of a right sectoral hepatic duct, either into the common bile duct or the cystic duct, increases the risk of injury during LC. This anatomic variation has also been reported as a surgical hazard for open cholecystectomy. Overall, anatomic variations and congenital abnormalities of the biliary tree may occur in up to 42.4% of patients. The aberrant right sectoral hepatic duct may be present in 4.6%–5.3% of operative cholangiograms [1]. The patient in the present case also had biliary anatomic variation with low insertion of a RPSD into the common bile duct. We were unaware of the aberration preoperatively and even during open conversion surgery.
An isolated sectoral duct injury presents a different problem compared with a common bile duct injury. Isolated sectoral duct injuries in particular may present a challenge for both diagnosis and management, because the biliary system remains connected to the duodenum, and only a section of the liver is left without proper drainage. Therefore, diagnosis is often elusive, as endoscopic retrograde cholangiopancreatography (ERCP) can be read as normal in the setting of continued biliary leakage. While classic common bile duct injury undergoes a conventional repair, the Roux-en-Y hepaticojejunostomy, the treatment of choice in this nonclassic injury is not well defined. But, many surgeons do routinely perform Roux-en-Y hepaticojejunostomy in order to reattach the right posterior section. Other options that have been reported include induced atrophy or surgical resection of the involved liver segment [45]. The treatment depends on the timing of the recognition of the type of injury. External biliary drainage should enable prompt control of the leak, eliminate the risk of sepsis and serve as a bridge for definitive repair. Biliary leak from an isolated bile duct is usually intractable because a noncommunicating fistula never closes spontaneously and continues to produce bile [2]. If the leak persists beyond approximately 8 weeks, treatment with Roux-en-Y hepaticojejunostomy is usually indicated [5]. However, reoperation can present a technical problem due to dense adhesion as well as high mortality and morbidity, therefore reoperation is an option that both surgeons and patients want to avoid whenever possible [267].
Endoscopic treatment, including sphincterotomy with a stent, is now widely accepted as another effective modality with which to manage biliary leak resulting from classic bile duct injury. Although ERCP is useful for identifying the site of a biliary leak and for treatment, it has a limitation in that the biliary leak must be from the main biliary system, such as the cystic duct or common hepatic duct. However, biliary leak from an isolated bile duct does not communicate with the main biliary system [6]. For this reason, nonoperative interventional treatment such as a biliary sclerotherapy can be a very attractive alternative because biliary sclerotherapy is known to induce atrophy of the infused hepatic segments with compensatory hypertrophy of the noninfused segments, as in portal vein embolization [7].
There are some reports on successful biliary sclerotherapy of biliary leaks from an isolated bile duct using ethanol or acetic acid as a sclerosing agent. Matsumoto et al. [8] reported a successful treatment of an isolated bile duct for a biliary-cutaneous fistula case with 11 sessions of ethanol infusion. In another report by Kyokane et al. [9], the isolated bile duct was treated with 6 sessions of ethanol infusion. However, Park et al. [7] reported that ablation of an isolated bile duct was successfully performed with 50% acetic acid in only 4 sessions. Ethanol is generally used as an injected agent percutaneously or angiographically for the treatment of various tumors because of its highly destructive properties, which lead to cell death by causing cell membrane lysis and protein denaturation [7]. In an animal study on selective intrahepatic biliary ethanol injection, ethanol destroyed the biliary epithelium, permeated parenchyma, induced hepatocyte degeneration, and resulted in compensatory hypertrophy of the noninjected hepatic lobe [9]. However, the desiccating action of acetic acid on protein-induced coagulation necrosis and the area of necrosis is significantly greater than that produced by ethanol if the concentration of acetic acid is greater than 20% [7]. Because injected acetic acid is easily diluted by the bile juice, the concentration should be higher. However, its effectiveness in the destruction of hepatocytes plateaued at a concentration of 50% [610]. For these reasons, we decided to use 50% acetic acid as a sclerosing agent to treat the isolated bile duct and the biliary leak was treated in 5 sessions.
In conclusion, a biliary leak from an isolated bile duct after cholecystectomy is intractable and the conventional surgical treatment is troublesome for both surgeons and patients. Acetic acid sclerotherapy can be considered a feasible and effective alternative for the surgical treatment of isolated RPSDs after cholecystectomy in selective patients who cannot undergo conventional surgical treatments.




 XML Download
XML Download