

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic cholecystectomy has become the gold standard treatment for gallbladder diseases in surgical practice, and now it is one of the most frequently performed procedures of general surgery. Recently, laparoscopy has become the preferred approach for a wide variety of abdominal surgeries due to reduced postoperative pain, rapid recovery, and improved cosmetic results compared with laparotomy. Although the laparoscopic surgical procedures are not completely risk-free, various complications may occur in 0.1%–10% of patients [1]. The most commonly reported complications are hemorrhage, bile duct injury, and bile leakage. Complications due to intra-abdominal pressure (IAP) resulting from pneumoperitoneum have not been well documented. Metabolic, immune and oxidative stress responses were minimal at 8–12 mmHg IAP, thus it has been considered as a safe pressure range for laparoscopic procedures [2]. In recent years, surgeons taken efforts to reduce the size, number, and placement of incisions to reduce abdominal wall trauma, thereby making single incision laparoscopic surgery a popular surgical procedure [3]. However, this new technique cannot be recommended as a standard operation for laparoscopic cholecystectomy [45].
Ischemia-modified albumin (IMA) has emerged as a sensitive biomarker in the evaluation of ischemia-based acute coronary syndromes, and was used in many other ischemic conditions [6]. In recent years, different studies have described the role of IMA as a new marker for diseases related to ischemia such as skeletal muscle ischemia, stroke, and pulmonary thromboembolism [78]. Several reports proved that ischemia induces a cascade of proinflammatory reactions that lead to the production of reactive oxygen species [910]. The aim of this study was to evaluate the effect of 2 different surgical techniques on systemic oxidative stress by using the serum oxidative stress marker IMA.
METHODS
Patients
This prospective study was conducted from November 2012 to December 2013 at the Department of General Surgery of our University Research Hospital. The study was carried out in accordance with the Code of Ethics of the Declaration of Helsinki. The study protocol was reviewed and approved by the Selcuk University ethical commitee (11/12–9). All patients were informed about the potential complications of the techniques, and written informed consents were obtained before enrollment. Surgical techniques were selected based on patients' requests only. In total, 70 patients who had been referred with benign gallbladder pathology were enrolled for this study. In this study, 21 patients underwent single incision laparoscopic cholecystectomy (SILC) and 49 patients underwent laparoscopic cholecystectomy (LC). Patients with a positive history of cardiovascular events and abdominal operation, other acute or chronic ischemic conditions such as stroke, transient ischemic attack, peripheral vascular disease, shock, and pulmonary diseases were excluded. Additional exclusion criteria were diabetes mellitus and smoking. Patients received no medications 1 week before surgery.
All operations were performed under general anesthesia by the same surgeon (HY). Prophylactic antibiotics and low molecular weight heparin were not administered preoperatively. A naso-gastric tube was placed to deflate the stomach before creating the pneumoperitoneum.
Operative technique
In SILC, the patient was placed in a supine position on the operating table with the legs spread in a slight Trendelenburg with the right side up. The surgeon was positioned between the patient's legs, the camera assistant was on the left side of the patient while the laparoscopic system lay on the right. Access was gained into the abdomen through an infraumbilical 20-mm incision. A multichannel SILS Port (Covidien, Mansfield, MA, USA) was introduced and pneumoperitoneum was established at an abdominal pressure of 12 mmHg. A 30° laparoscope (Karl Storz, Tuttlingen, Germany) was inserted and the abdominal cavity was routinely examined. The infundibulum was grasped with a forceps and retracted slightly upward to expose Calot triangle. The cystic duct and the cystic artery were carefully dissected and clipped. Retrograde cholecystectomy was carried out with an ultrasonically activated scalpel (Harmonic Scalpel-Ethicon Endo Surgery, Cincinnati, OH, USA). After a thorough observation of the hepatic bed the gallbladder was removed from the incision line. At the end of surgery, the umbilical access was closed with a number of 0 polyglactin running sutures. The skin was closed using 4-0 Monocryl in a running subcuticular fashion.
Conventional LC was performed by 4 trocar replacements (10-mm optic at the umbilicus, 10-mm trocar in the epigastrium and two 5-mm trocars in the right upper abdomen).
Blood collection
Blood samples were drawn before operation (basal), and 45 minutes (early), and 24 hours (late) after the operation. Blood samples were collected directly into serum separator tubes (VACUETTE, Greiner Bio One GmbH, Kremsmünster, Austria). After coagulation, centrifugation process at 1,500 g for 10 minutes was performed. Sera were separated, stored in aliquots, and kept frozen at −70℃ until analysis.
Measurement of IMA
Serum albumin levels (g/dL) using the colorimetry method were assayed with Advia 2400 analyzer (Siemens Healthcare Diagnostics, Tarrytown, NY, USA). The levels of serum IMA were analyzed using the rapid and colorimetric method developed by Bar-Or et al. [11]. The results were reported as absorbance unit. Serum IMA levels can vary with serum albumin levels. Therefore, the adjusted IMA levels were calculated with the formula suggested by Lippi et al. [12]. Albumin-adjusted IMA levels were expressed as individual serum albumin concentration/median albumin concentration of the population x IMA value.
Statistical analysis
SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical evaluation of the data. Categorical variables were analyzed by chi-square test; continuous variables were analyzed by the Mann-Whitney U-test and Paired t-test. Statistical significance was defined as a P-value less than 0.05.
RESULTS
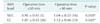
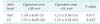
During the study period, a total of 70 patients with benign gallbladder disease underwent cholecystectomy. SILC and LC procedures were performed in 21 and 49 patients, respectively. Preoperative characteristics of the patients are presented Table 1. There was no statistically significant difference between the 2 groups with regard to the age, sex, body mass index, American Society of Anesthesiologists physical status classification, and preoperative diagnosis. All SILC procedures were completed successfully without conversion to LC or open repair, and no additional port was required in both groups. Compared with the LC group, the mean operative time was longer in SILC group (37.5 ± 12.5 minutes in the LC group and 44.6 ± 14.3 minutes in the SILC group). But, there was no statistically significant difference between the groups. Although the SILC group was composed of younger patients, the difference was not statistically significant. Preoperative IMA levels were not different in SILC and LC groups, and there was no significant difference between postoperative IMA levels at 45 minutes and 24 hours (Table 2). Operative technique did not effect the IMA levels but the groups were compared in terms of operative time; the early (45th minute) measurement of IMA levels were increased by prolonged (>30 minutes) operative time (Table 3); the subsequent measurement (24th hour) of IMA levels were not different in patients with prolonged surgical time (Table 4).
DISCUSSION
The principal finding of this study is that surgical technique did not effect the IMA levels related with tissue ischemia, and the second finding is that prolonged operative time could cause a significant increase of IMA levels due to pneumoperitoneum. Laparoscopy has some potential advantages over laparotomy that include reduced postoperative pain, shorter operative time, reduced hospital stay, faster recovery, decreased adhesion formation, and smaller scar with better cosmesis [13]. Since its introduction in surgical practice, LC has become the gold standard, and is now one of the safest procedures of general surgery. Single-incision laparoscopic surgery (SILS) was first applied to decrease the invasiveness of conventional laparoscopy. Recently, it has been a more frequently applied technique in surgery. In this study, we have attempted to evaluate single-port cholecystectomy and traditional 4-port cholecystectomy with respect to postoperative tissue ischemia. The study design was prospective. But, there was a limitation of this study, namely, the choice of surgical technique to be used was based on patients' demands. The groups were not randomized. These limitations should be kept in mind while evaluating the study results.
Some of the complications may be related to pneumoperitoneum and carbon dioxide. Intra-abdominal insufflation of carbon dioxide is the most widely used technique for creating working space during laparoscopy. It is important to keep the abdominal pressure under 12 mmHg because IAP greater than 12 mmHg may cause pathological changes in the cardiovascular system, hemodynamic parameters, pulmonary system, and renal function [14]. It has been known that increase of IAP causes a reduction in splanchnic blood flow resulting in biochemical evidence of oxidative stress and histological evidence of tissue injury [15]. Many studies have been published to prove single-incision cholecystectomy has reduced pain, and better cosmesis [1617]. However, recent studies have demonstrated that SILC procedures have similar results with LC in terms of pain and complication rates. There is no investigation on the effects of surgical technique on ischemic conditions. Our results showed that surgical technique or number of incisions have no effect on tissue ischemia. Tissue ischemia in patients undergoing LC is associated with the increase of IAP.
Previous studies have demonstrated that CO2 pneumoperitoneum during laparoscopy has some adverse effect in safe IAP ranges. The critical time to ischemia has been determined as 30 minutes after CO2 pneumoperitoneum [18]. Therefore, 2 additional groups were created in terms of operative time. Should the peritoneum absorb carbon dioxide into the circulation, it may cause acidosis. Acidosis due to a direct effect of carbon dioxide gas could alter serum oxidative stress markers. In this study, we monitored carbon dioxide levels during the operation. The operations were performed under general anesthesia with mechanical ventilation. The minute volume of ventilation was increased automatically and was adjusted to end-tidal carbon dioxide pressure. End-tidal carbon dioxide pressure level was set as 35 mmHg and excess carbon dioxide was excreted through the lungs without causing acidosis. However, volatile anesthetics under mechanical ventilation could induce an inflammatory response. A similar anesthesia protocol was followed for all patients to standardize the groups.
IMA was introduced as a serum biomarker and increase of IMA levels in patients with acute coronary syndrome has been used for an early marker of myocardial ischemia [6]. However, increased IMA concentrations do not seem to depend purely on myocardial involvement. Serum IMA levels were found to be increased in non-myocardial ischemic conditions such as skeletal muscle ischemia, stroke, and various type of malignancies [71920]. The cobalt-binding capacity of albumin reduces, because of oxidative free radicals during ischemia and this new chemically changed albumin can be measured with albumin cobalt binding test. High values of IMA are closely related to ischemic conditions. Recent studies shows that IMA is more sensitive than other markers (malondialdehyde, total antioxidative status, total oxidant status, oxidative stress index) in early detection of systemic oxidative stress in operative laparoscopy [18]. In this study, prolonged pneumoperitoneum has led to significant increases in early IMA levels. However, the IMA levels 24 hours after the operation were not different. This indicates that the resolution of tissue ischemia occurs in the early postoperative period.
In the majority of studies, SILS groups have a longer operative time because of the very close proximity of the instruments with limited triangulation and limited motion of laparoscope [2122]. The surgeon's experience is very important in reducing the operative time. Our study surgeon and camera assistant were experienced in SILS with 500+ cases. Therefore, operative times of the groups were found to be similar in our study.
Analysis of patient demographics demonstrated that patients undergoing SILC were significantly younger than patients undergoing LC. SILC was favored by young patients due to the better cosmetic results.
In conclusion, based on the present findings, SILC seems to be a safe technique with remarkable cosmesis. The operating time is long initially, but it shortens as surgeons become more experienced with the procedure. Prolonged operative time can cause temporary tissue ischemia in all laparoscopic procedures. This ischemic condition is also improved within the first 24 hours. The sample size was limited in this study. Nevertheless, our preliminary findings should act as a stimulus for further studies involving larger samples and other oxidative stress markers.


 XML Download
XML Download