

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The numbers of less invasive endovascular therapies continues to increase, driven by patient preference and outcome data in almost every vascular lesion. In the United States, intervention for lower extremity lesion increased by 300% over the last 10 years [12]. Although vascular practice in different countries varies, this global paradigm shift has heavily impacted Korean vascular practice recently. According to Korean Health Insurance Review & Assessment Service data, endovascular therapy numbers already surpass open vascular surgery [3]. The hybrid vascular surgery room has become popular in Korea, with variable intervention and hybrid procedures undergone therein [4]. Fluoroscopy is essential in providing image guidance for most endovascular procedures. Because of the evolution in device technology and skill, fluoroscopy time continues to increase with more complex procedures such as endovascular aneurysm repair (EVAR). Since mobile C-arm fluoroscopy has become more available in most hospitals, in Korean hybrid vascular units are usually made up of mainly radiologic equipment. Therefore, vascular surgeons performing endovascular procedures, as well as attending vascular scrub nurses, are at risk of exposure to potentially hazardous ionizing radiation. Because of this radiation concern, the Society of Vascular Surgery already published safety guidelines in 2011 [5]. However, even with these national principles, about half of young vascular surgeons have had no formal radiation safety training [6]. Korea has been placed in the worst position relatively because there are no society guidelines yet, especially concerning current popular mobile C-arm equipped hybrid vascular rooms. There have seldom been studies regarding radiation hazards so far. The aims of this study are to assess the current levels of professional exposure in the hybrid vascular suite and to estimate the corresponding levels of long-term lifetime attributable cancer risks of vascular staff based on direct radiation measurement.
METHODS
Fluoroscopy and subjects
A prospective study was undertaken in 71 consecutive patients (53 men and 18 women) who had an angiogram performed during hybrid vascular operation in our vascular surgery division. The mean age of subjects was 70.8 years (range, 34–91 years) and the mean body mass index was 21.6 kg/m2 (range, 15.4–29.1 kg/m2). The study period was 6 months from November of 2011. All vascular interventional procedures were performed in our vascular hybrid surgery room on the central operation floor. The patient was placed on the radiologic carbon surgical table (Macquet Alphamaxx, Maquet, Rustatt, Germany) and intervention was performed under fluoroscopic guidance using OEC 9900 Elite MD mobile C-arm (GE OEC Medical Systems Inc., Salt Lake city, UT, USA). The C-arm was equipped with an image intensifier at the size of 23 cm2, an additional filter at 3 mm A1+0.1 mm Cu and a Carbon fiber X-ray grid. An auto-exposure controller was used for the exposure parameters, such as tube voltage, tube current, and exposure time as a continuous fluoroscopy, and the range of tube voltage (KV range) was 40–120 kV, while the range of the tube current (mA range) was 0.44–20.2 mA. The distance between the X-ray tube focus to the patient was somewhere between 30 and 50 cm depending on the thickness of the patient or purpose of the procedure.
Direct vascular surgeon and nurse exposure calculation
In order to measure the direct radiation exposure of the operating vascular surgeon, an optically stimulated luminescence (OSL) dosimeter (InLight/OSL NanoDot dosimeter, Landaure, Glenweek, IL, USA) was attached to the radiation protecting garments (Fig. 1). The low limit measurable dose of OSL was 100 µSv, the energy range was between 5 keV and 20 MeV, and the accuracy was ±5% standard. The OSL was attached on each inner and outer side of the lead goggle, thyroid protector, apron (breast level) and apron at the position of gonad being worn by the operator (Fig. 2). For detection of radiation expose to scrub nurses who always stand next to the operator just slightly further from the C-arm, OSL was also placed on the outer and inner sides of the chest apron being worn by the scrub nurses who participated in vascular interventional procedures. Although the attending scrub nurse changed during the study period, nursing staff maintained the basic principle to always wear the same OSL attached lead apron. OSLs were never removed or used in a different position during study period and were sent to a reading institution after 6 months to analyze the dose information. The results from the reading were described as a dose. Effective dose of the surgeon was calculated in accordance to the equation of Niklason et al. [7]. For the lifetime attributable risk (LAR) of cancer for the staff, Biological Effects of Ionizing Radiation (BEIR) VII Report was used as reference [8]. The number of solid cancer incidences per 100,000 persons when exposed to a dose of 10 mGy annually from the age of 18–65 was used in this report. Thus, the same method was applied for risk evaluation for vascular surgeons in this study. However, it should be noted that in this study, the risk of cancer incidence was estimated by the assumption that the dose for 1 year continued for up to 65-year-old for surgeons.
Calculation scatter X-ray
During fluoroscopy, scatter radiation is another important hazardous radiation exposure to surgeons or nursing staff. The patient is the most significant source of scatter radiation. Since the scrub nurse is usually located further from the C-arm than the surgeon, it is believed that radiation hazards would be lower. However, the scatter radiation effect is unpredictable, so we proceeded to perform another test to measure scatter radiation. During mobile C-arm fluoroscopy operation over an anthropomorphic phantom model (Whole body phantom PBU-60, Kyoto Kagaku Inc., Kyoto, Japan) laid on a surgical table, radiation dose was measured using personal gamma radiation dosimeter, Ecotest CARD DKG-21 (Ecotest Inc., Lviv, Ukraine) (Fig. 3). Data was collected at three distances (20, 50, 100 cm) and 3 angles (horizontal position, downward tube direction 45°, upward image intensifier direction 45°). Each measurement was made every 1, 3, 5, 10 minutes. Fluoroscopy exposure condition was measured using automatic settings by manufacturer. In addition, the distance between the X-ray tube and the image intensifier was 100 cm.
RESULTS
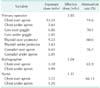
During the 6-month study period, 71 patients underwent vascular intervention in our hybrid vascular operation room. The mean age of patients was 70.84 ± 12.22 years and body mass index was 21.57 ± 2.96 kg/m2. The characteristics of subjects are listed in Table 1. The details of vascular procedures are listed in Table 2. The mean fluoroscopy time is 11.86 minutes (maximnum. 51.4 minutes) and the total time was 842 minutes. Balloon angioplasty with or without stent insertion was the most frequent procedure and EVAR took the longest fluoroscopic time. Planned therapeutic failure with no device deployment and simple diagnostic angiography were classified as simple angiography procedure.
Vascular surgeon dose and cancer risk
The 6-month effective dose of the operator's OSL dosimeter from vascular interventional procedures was 3.85 mSv, and its annual exposure dose was estimated as 7.70 mSv. During the same period, scrub nurse's exposure dose over and under apron was 3.72, 1.26 mSV. Effective dose was 1.31 mSV, so annual dose is assumed to be 2.62 mSv. The dose measured from the outer side of the lead apron covering the gonadal gland of the primary operator was 8.61 mSv and at the eyes was 6.86 mSv presenting in the direction toward the gonadal gland of the operator was more exposed than toward the face. When the attenuation rate was identified by comparing the doses measured from the inner side and the outer side of radiation protectors, the attenuation rates of aprons and thyroid protectors containing 0.5 mm of lead (Pb) were 74.6% and 60.6%, respectively, while the attenuation rate of goggles containing 0.07 mm of lead (Pb) was 70.1% (Table 3). The results of LAR of cancer was presented, as shown in Table 4, as calculated by estimating the annual exposure dose of primary vascular surgeons, which was 7.7 mSv. When assuming that a surgeon was continually exposed to radiation working from 18 years old to 65 years old, all cancer incidences of the male vascular surgeon correspond to 2,355 persons per 100,000 persons, which deems that 1 of 42 persons is likely to have all cancer incidences. In addition, if exposed to radiation doses of 7.7 mSv per year continually, the mortality would be stated as 1309 per 100,000, which is 1 of 76 persons (Table 4). For female scrub nurses, all cancer incidences per 100,000 persons are 795 persons, converting to 1 of 89 persons, and the mortality of 2.62 mSv would be 1 of 160 persons, respectively.
Procedural exposure
According to the International Commission on Radiological Protection (ICRP) recommendations, the annual occupational dose limit is 20 mSv averaged over 5 years, with no more than 50 mSv in any one year [9]. Total fluoroscopy time of 71 procedures was 842 minutes and effective dose was 3.85 mSv. Based on these results, the annual upper limit of fluoroscopy time would be 4,674 minutes from 394 interventional procedures. Since EVAR is a more complicated procedure, the mean fluoroscopy time was 30.4 minutes, which is about 3 times longer than angioplasty ± stent by 11.9 minutes. Thus, the annual vascular work limitation would be 154 EVARs and 393 angioplasties.
Scatter ray measurement
Cumulative dose with Ecotest CARD DKG-21 on a phantom model in the middle of the C-arm beam field for 1, 3, 5, 10 minutes are 3.5, 11.2, 18.8, 37.8 mSv, respectively. The 10 minutes dose at 20 cm horizontal was 0.162 mSv and 45° degree in the downward to tube direction was 0.698 mSv, upward image intensifier direction was 0.073 mSv each (Table 5). If the 10-minute cumulative dose of upward direction is assumed to be 100%, the horizontal dose is 23.2%, and the downward direction point is 23.2%, relatively. The 10-minute dose at 100-cm distance at each angle were horizontal 0.004, downward 45° 0.009, upward 45° 0.003 mSv. Based on this observation, it is confirmed that during fluoroscopy, operator's radiation exposure in the gonadal area is greater than the eye area. The cumulative dose was inversely proportional to the square of distance of the radiation beam field.
DISCUSSION
During the last few decades, minimally invasive endovascular therapy has become main stream in all types of vascular pathology including aortic aneurysm and peripheral arterial occlusive disease. Korean vascular practice has rapidly changed also; according to the national health database, peripheral arterial balloon angioplasty has increased by threefold compared to 10 years prior [3]. However, since most endovascular therapies require the use of ionizing radiation for guiding procedures, radiation safety concerns for the vascular team has been growing. In Korea, mobile C-arm fluoroscopy equipment has become more popular than a fixed angiogram system because of cost benefit; however, there is the belief that the mobile C-arm may be more hazardous in terms of radiation exposure. These changes in working environment increased concern not only for vascular surgeons but also for scrub nurses, especially young female of child-bearing age. Although since 1996, in Korea, occupational radiation has been relatively well monitored and recorded by making it a legal requirement for all radiation workers to wear a thermoluminescence dosimeter (TLD), occupational radiation data in hybrid vascular operation rooms has rarely been studied Korea so far. Especially, young vascular surgeons' cumulative radiation hazards will becomes more problematic in the future because they are exposed to radiation earlier, since fellowship courses, where endovascular procedures have increased by over 400% during the previous decade [10]. Although much of the knowledge used in radiation safety comes from studies of high-dose exposures, such as atomic bomb survivors, it is thought that the risk of malignancy after low-dose X-ray exposure is approximately directly proportional to the cumulative dose received [11]. The most commonly discussed deterministic injuries include skin and eye injuries, and the cancer is the most concerning stochastic injury. Usually, the more complex procedure, the more radiation exposure is inevitable for the operator, such as EVAR, although the benefit for patients is higher in procedure related mortality [12]. According to Bannazadeh et al. [13], EVAR for infrarenal aortic aneurysm received the highest effective dose (109 mSV) compared to lower extremity intervention (47 mSv). Also, longer intervention creates higher skin dose in patients. In our study, EVAR procedure showed the highest effective dose of 27.0 mSv and the longest mean fluoroscopy time of 30.4 minutes. Based on our results considering the ICRP yearly occupational guideline 20 mSv, it is assumed that the maximum safe annual EVAR numbers would be 154 operations and 393 balloon angioplasties per surgeon. Any high volume center going over these procedure numbers should take personal radiation workload into consideration. In another study, median yearly effective dose for vascular surgeons for body, eye, and hand were 0.20 mSv (range, 0.13–0.27 mSv), 0.19 mSv (range, 0.10–0.33 mSv), 0.99 mSv (range, 0.29–1.84 mSv), respectively [14]. Lipsitz et al. [15] reported that yearly total effective dose for vascular surgeons during EVARs with mobile fluoroscopy were 1.52 mSv for body, 7.77 mSv for eye, 18.69 mSv for hand. Although the present results for yearly dose of 7.7 mSv did not exceed the dose limit of 20 mSv for workers designated by ICRP, which is 150 mSv for eye lens and thyroid, and 500 mSv for hands and limb, it should not be ignored [9]. Because cumulative dose will keep rising over time with procedures, it is another important factor in radiation inducing cancer. Lifetime attributable cancer risk assessment in BEIR VII report, is one of the more well known risk assessments. According to this report, when exposed continuously to 10 mSv on a yearly basis from ages 18 to 65 years old, cancer incidence was 3,059 for male and 4,295 for female. Venneri et al. [16] had reported that the early exposure dose for interventional cardiologists was median 3.3 mSv (range, 2.0–19.6 mSv), cardiac electrophysiologists was median 4.3 mSv (range, 3.5–6.1 mSv), and risk of all cancer incidences was 1 out of 192 persons. Although there are study limitations in our results, exposure dose for vascular surgeon was higher than that for cardiologist, and it would be a higher cancer incidence [16]. The assumed mortality from 47 years of radiation from age 18 years old would be stated as 1,309 per 1,000,000 persons. Considering jobs with the highest fatalities in the U.S., loggers showed 128 deaths per 100,000 workers [17], the mortality number from radiation is considerable. During vascular intervention, radiation shields such as lead apron and goggle are used. Even so, when performing prolonged procedures, there is no way to avoid exposure to radiation. If not using the proper protection tools, or not adjusting exposure time adequately, the eyes or skin, thyroid and gonadal gland can experience impairment due to X-ray radiation scatter within a few years as reported [18]. Also, in our study if the 10-minute cumulative dose of upward direction is assumed to be 100%, the horizontal dose is 23.2%, and the downward direction point is 23.2%, relatively. Thus, the surgeon's gonadal direction is more hazardous than the eyes. The shielding rate of radiation protection identified by this study was about 74.6% and 60.6% from 0.5-mm-thick apron and thyroid protector, respectively, and was 70.1% from 0.07-mm Pb goggle indicating the radiation shields cannot block the scattered rays 100%. During hybrid vascular surgery wearing surgical loupes hinder the use of lead goggles, so in this situation safety principles are ignored. Yearly exposure dose to outside and inside of goggles were 13.7 and 4.1 mSv, respectively. Although ICRP has stated that the threshold for radiation induced cataract formation is 4 Gy for fractionated exposures [19], there is some evidence that the lens may be more sensitive than previously thought. In fact, during the 2004 Radiological Society of North America meeting, Haskal [20] screened 59 interventional radiologists and found that 8% had posterior subcapsular cataracts. Radiation-induced cataracts have been described in interventional radiologists with lens doses approaching 150 mSv/yr [21]. In our study, we did not measure radiation to operator's hand due to study design. According to another study, the annual dose for an interventional doctor performing 100 peripheral angiographic procedures per year is estimated at 40 mSv to the hands and fingers and 30 mSv to the eye/head [22]. This means that during a 40-year career, the total dose to the hands and fingers can start to approach the threshold dose for radiation-induced skin injury [22]. Since procedures taking place close to image intensifiers are becoming prolonged, vascular surgeon hand protection is becoming more important than before. So far, many international cardiovascular societies published patient, medical practitioner radiation safety guidelines and have urged keeping to strict regulation [52324]. Even with these efforts, 74% of young trainees who are the most vulnerable to cumulative long-term radiation exposure were unaware of policies such as as low as reasonably achievable. There is groundless belief that a mobile C-arm could be more hazardous than a fixed angiogram system. However, in our study direct dose measurement with Ecotest CARD DKG-21, 100-cm distance exposure dose was very low at 0.004 mSv. Fossaceca et al. [25] also reported that radiation dose in EVAR is substantially less with a modern portable C-arm than a fixed angiogram system. Since the scrub nurse is usually located further than the operator during fluoroscopy, it is believed that being further than 100 cm from the C-arm would be a safe distance. In addition, nurses' daily work shifts change; thus, radiation risk would be much lower than for vascular surgeons. So far, the Korean Vascular Surgical Society has not yet published radiation protection regulations. Therefore, the goal of regulating proper protection devices and monitoring the annual effective dose of personnel who attend endovascular procedures in hybrid vascular rooms is urged.
Our study has several limitations. Since the risk of cancer incidence at the effective dose for surgeons was calculated by using BEIR VII Report, it is an assumption based on daily exposure. Also, this study had ruled out many potentially personal, mechanical, and environmental factors that can affect the effective dose in the course of surgical procedures. Finally, procedural characteristics are dependent on each vascular center's experiences and skill, so there is limitation for generalization in our results. Even so, this is the first report of direct measurement of radiation dose in hybrid vascular rooms with a mobile C-arm so it can offer valuable reference to the current vascular practice in Korea in terms of radiation safety.
In conclusion, the annual effective dose for vascular surgeons and scrub nurses performing mobile C-arm fluoroscopy was still below the ICRP occupational guidelines. However, proper protection devices are necessary to decrease inevitable radiation hazards such as cancer incidences.







 XML Download
XML Download