

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic appendectomy (LA) has been accepted as the gold standard procedure for complicated or uncomplicated acute appendicitis [1]. The advantages of LA over traditional appendectomy are better cosmetic results, less postoperative pain, fewer postoperative infections, shorter hospitalization, and earlier recovery [23]. Conventional laparoscopic appendectomy (CLA) uses 3 ports during the surgical procedure. The recently developed single port technique has improved this minimally invasive surgery to an even higher level. Most of the single port appendectomy studies did not reveal any other advantages other than technical feasibility and cosmetic results. Even though there is an advantage to the reduction of surgical sites using a single port technique, disadvantages include a larger incision diameter, which leads to a wider fascial defect, more postoperative pain, and longer operation time. One of the other disadvantages of the single port technique is higher operation cost [3456]. Two-port laparoscopic appendectomy (TLA) is a minimally invasive surgical procedure, which results in a shorter incision, less postoperative pain and a better cosmetic result. There are many studies that have used this surgical technique [78].
We performed TLA with the help of an additional needle grasper (percutaneous organ holding device). We hypothesized that using fewer surgical ports with this technique would lead to less surgical trauma, less postoperative pain, and better cosmetic results. In order to support this theory we compared the results of using TLA with a needle grasper with CLA.
METHODS
This retrospective study was performed at Istanbul, Lutfiye Nuri Burat State Hospital during February 2015 to November 2015 with 2 surgeons experienced in laparoscopic surgery. We retrospectively analyzed the 70 patients with acute appendicitis who underwent laparoscopic procedures. Patients were diagnosed with acute appendicitis using abdominal ultrasonography (55 patients) or CT (15 patients). LA techniques were determined by the surgeon's preference. Patients were divided into 2 groups: group 1 (CLA), and group 2 (TLA). Thirty-two patients undergoing TLA and 38 patients undergoing CLA were included in this study. Patients with complicated appendicitis, such as generalized peritonitis and plastrone appendicitis, were excluded from the study. The possible surgical methods, such as TLA, CLA, and open appendectomy, were explained to the patients preoperatively. They were also informed about the risk of conversion from the laparoscopic procedure to an open technique during surgery. Informed consent forms were obtained from all patients before the surgery.
Age, sex, height, weight, body mass index (BMI), and comorbid diseases of the patients were recorded. Duration of operation, duration of hospitalization, postoperative pain levels (visual analog score, VAS), and time to enteral feeding were evaluated and recorded. Postoperative pain levels were evaluated using VAS at 1, 6, 12, and 24 hours postoperatively on a scale of 0 to 10.
This study was approved by the Haseki Research and Training Hospital Ethics Committee on November 11, 2015 (approval number: 274).
Surgical method
Patients were prepared with a standard preoperative anesthesia procedure. Operations were performed with a left-positioned surgeon and an assistant (scopist). The operation was started after the standard general anesthesia. In group 2 (TLA), a 1-cm skin incision was performed under the umbilicus and the abdomen was entered using a veress needle. Pneumoperitoneum with 14-mmHg CO2 pressure was obtained and a 10-mm trocar was inserted into the abdomen. A 0-degree 5-mm optical camera was inserted through the umbilical trocar and a 5-mm trocar was inserted through the suprapubic area. Patients were placed into the Trendelenburg position angled 15 degrees toward the surgeon. Diagnostic exploration was performed and acute appendicitis was verified. A needle grasper (Percutaneous Organ Holder Device, Suture Grasper Closure Device, Mediflex Surgical Products, Islandia, NY, USA) was inserted through McBurney's point (Fig. 1A, B). The appendix was held and secured using the needle grasper. The appendix was manipulated easily and successfully with an endograsper (Fig. 2A). The mesoappendix was cauterized and cut with endoligasure (LigaSure, Covidien, Boulder, CO, USA). An endoloop was inserted through the 5-mm trocar and passed from the tip to the neck of the appendix and sutured (Fig. 2B). A clip was inserted above the surgical knot with endoclips and cut. The optical camera was then inserted through the 5-mm suprapubic trocar and an endobag was inserted through the 10-mm umbilical trocar. The surgical specimen was placed into the endobag and removed from the abdomen. After the surgical procedure was completed, the abdominal fascia was closed with 2/0 vicryl, and the skin was closed with 4/0 intracutaneous vicryl sutures.
In group 1 (CLA), a 1-cm skin incision was performed under the umbilicus and the abdomen was entered with the help of veress needle. Pneumoperitoneum with 14-mmHg CO2 pressure was obtained and a 10-mm trocar was inserted into the abdomen. A 0-degree 10-mm optical camera was inserted through the trocar and two 5-mm trocars were then placed in a triangle-shaped pattern. The subsequent appendectomy was performed using the conventional technique. The abdominal fascia and skin were then closed with absorbable sutures.
Data evaluation
Age, sex, height, weight, (BMI), American Association of Anesthesiology Score (ASA) score, preoperative leukocyte number, duration of operation, VAS for pain, duration of hospitalization, postoperative complications, postoperative pain, and cosmetic satisfaction were recorded. All patients received paracetamol (1 g/8 hr) IV as the standard analgesic treatment and evaluated for pain postoperatively. The wound satisfaction score (WSS; very unsatisfied, 1; unsatisfied, 2; acceptable, 3; satisfied, 4; very satisfied, 5) was recorded for each patient in the TLA group 20 and 30 days postoperatively to assess the patient's satisfaction with their scar. Using the VAS, the worst pain possible was scored as "10 points" and no pain was scored as "0 points", with variable degrees inbetween. Evaluation was performed at 1, 6, 12, and 24 hours postoperatively by an uninformed anesthesiologist. Postoperative complications, wound infections, stump leakage, ileus, and intraabdominal abscess formation were investigated and recorded.
Statistical analysis
Statistical analysis was performed using the SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Quantitative variables were expressed as mean ± standard deviation or range, whereas categorical variables, such as number of patients, were expressed as a percentage. The normality of quantitative variables was analyzed by the Kolmogorov-Smirnov test and normally distributed variables were compared with Student t-test or the Mann-Whitney U-test when they were not normally distributed. Categorical variables were compared by chi-square or Fisher exact test. Values were considered statistically significant when P < 0.05.
RESULTS
We retrospectively investigated the hospital records of 32 patients that underwent TLA and 38 patients that underwent CLA. Demographic features (Age, sex, weight, height, BMI, ASA) of these 2 groups were statistically similar (Table 1). There were no comorbid conditions, such as hypertension, diabetes mellitus, or chronic obstructive pulmonary disease, in these 2 groups.
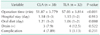
There was 1 patient in the TLA group and 2 patients in the CLA group that presented with perforated appendicitis. In the TLA group, 32 patients were successfully operated on and there was no need for conversion to the conventional method or open surgery. In the CLA group, 38 patients were successfully operated on with no need for conversion to open surgery. There were no statistically significant differences for preoperative leukocyte number, duration of hospitalization, time until enteral feeding, and complication ratio. There was a significant difference in operation time between the groups, with the mean duration of operation calculated as 57.03 ± 3.814 minutes in the TLA group, and 51.87 ± 3.779 minutes in the CLA group (P < 0.001). Hospitalization time was 1.15 days for the TLA group and 1.18 days for the CLA group with no significant difference (P = 0.913) (Table 2).
In the postoperative pain evaluation, VAS was lower at 1, 6, 12, and 24 hours in TLA group, but the only significant difference was observed at the 12 hours in the TLA group (P < 0.001) (Table 3).
In the TLA group, the cost of the needle grasper was approximately $70. In the CLA group, the cost of the additional trocar was approximately $77.80 and the basic endoclinch was $155.60. The mean total hospital cost for TLA group was calculated as 490.68 ± 16.48, while the mean total hospital cost for CLA group was calculated as 696.36 ± 13.42. This difference was statistically significant.
We encountered postoperative infection in 1 patient in the TLA group and 3 patients in the CLA group. We observed infection at the periumblical incision region for one patient in the TLA group and one patient in the CLA group. There is no statistical difference between the 2 groups (P = 0.231), and all patients recovered with medical treatment only. We placed hemovac wound drainage for 2 patients in the TLA group and 4 patients in the CLA group. Drainage tubes were removed during the first postoperative day. With one patient in the CLA group, who presented with perforated appendicitis, we observed an abscess in the pouch of Douglas. The abscess was drained by ultrasound-guided catheter. The catheter was removed on day 7 after drainage. We did not encounter any other complications in either group and all patients recovered successfully.
There was no significant scar from the needle grasper in the TLA group at postoperative day 20. All patients were satisfied with the cosmetic results (WSS, 4.46).
DISCUSSION
Technological advancement has opened a new era in medicine. Due to improvements in the laparoscopic literature, operations have progressed into single incision laparoscopic surgery (SILS) port and robotic surgery very rapidly. Many investigators have developed different techniques using natural hole transluminal endoscopic surgery. Laparoscopic appendectomies via vaginal approach have also been reported [910], but there are many risks for these procedures. Umbilical access laparoscopic procedures are the standard method for intraabdominal surgeries. Laparoscopic appendectomies are usually performed via umbilical access. There are many techniques for laparoscopic appendectomies: standard multiport LA, single port LA, and two-port LA are the transumblical methods. Standard LA is a surgical procedure using 3 ports. SILS port LA is a surgical procedure using a single-port, which has 3 or 4 internal lumens. In the SILS port procedure, a 2-cm incision is required, which may result in more postoperative pain and increased infection risk. Many studies have reported more postoperative pain using SILS port technique [111213]. In one study, Mayer and colleagues reported less postoperative pain in the SILS group [14].
When compared to using a SILS port, the described minimally invasive technique can be performed more easily due to better angulation of the instruments. In this technique, a percutaneous organ holder device may function as a grasper [15]. With the help of this needlescopic device, postoperative pain and scar formation may be minimized. In our study, we observed less postoperative pain in the TLA group at 12 hours compared with the CLA group. Operation time was also shorter in the CLA group. The reason for this difference is thought to be due to the difficulty in holding the appendix with the needle grasper caused by severe inflammation and edema, which led to accidental release of the appendix during manipuation.
In a recent meta-analysis study comparing the CLA and needlescopic appendectomy techniques, mini-laparoscopic appendectomy was found to be a safe and effective method, but led to longer duration of operation and higher conversion rates. There were no differences in hospitalization time [16]. In our study, we found no differences in hospitalization time and conversion rates between the 2 groups.
The most important aspect for the SILS port appendectomy and 2-port appendectomy is proper positioning for mesoappendix dissection. In order to cauterize and cut the appendicular artery during dissection of the mesoappendix the appendix should be properly retracted. There are many defined techniques to achieve this position. A study by Roberts [17] defined the "puppeteer technique" as a suture going from the right iliac fossa and retracted by the left hand of the surgeon. Using this defined novel "puppeteer technique," a "pulley" was used in the form of an intraabdominally placed loop through the abdominal wall as an axle to raise the appendix with a string. The tool is positioned by the surgeon from outside the abdomen, similar to a puppeteer moving the limbs of their puppets. The procedure using the puppeteer technique was performed successfully in 13 of 14 cases with less pain and better cosmetic results.
In a study by Yeung [18], another technique was described for stabilization of the appendix with the help of external suture at the right iliac fossa, known as "The intravenous catheter at McBurney's Point." However, because of the harsh holding and manipulation of the appendix during this technique, any inflammation leads to an increased risk of damage and leakage of contents from the appendix. Using this technique, the surgeon uses an intravenous catheter to insert a needle into the abdomen and retracts the appendix to the abdominal wall, followed by appendectomy. This procedures was performed successfully in 14 of 15 cases without complications. It was emphasized that McBurney's point is ideal for less risk of infection and fewer complications.
In a study by Ates et al. [19], the mesoappendix was stabilized to the right iliac fossa by a transparietal suture. This study used a single port LA technique, with a suture placed through the right inferior quadrant into the peritoneal space and inserted through the mesoappendix to secure the appendix to the abdominal wall. They reported better cosmetic results using this technique with less surgical tools inserted into the abdomen.
Another case series study used the 2-port LA technique and stablized the appendix to the abdominal wall by a suture [20]. A suture was tied in a loop to the anterior abdominal wall in the right lower quadrant, which was subsequently used as an axle. A suture was then placed on the appendix and pulled through the port to remove it from the abdomen. This technique allowed for better exposure of the base of the appendix without using a third port. The mesoappendix and appendix were stabilized and removed from the abdomen in an extracation bag.
In our study, for the TLA group, we inserted a needle grasper (percutaneous organ holder device) with the left hand of the surgeon at McBurney's point to hold the appendix for retraction, which has been proven as a safer point by many studies. The surgeon may manipulate the position of the appendix using the needle grasper in their left hand. The mesoappendix was cauterized by endoligasure, entering from the suprapubic trocar, and the appendix was skeletonized. The appendix was sutured at the neck using an endoloop, entering from the suprapubic trocar, and subsequent appendectomy was performed. In our study, we did not encounter complications such as appendix perforation or organ perforation due to use of the needle grasper. We did not observe postoperative pain or infection at the entrance point of the needle grasper. The diameter of the device is 2.1 mm and there is no need for an extra incision for needle insertion. The reason for using McBurney's point in our study was increased safety and decreased risk of infection [17181920]. With the help of the camera light, instrument insertion into the abdomen has become easier and safer. With the help of the needle grasper, which is inserted at this point, the appendix was held and retracted, and the mesoappendix was cauterized with endoligasure and skeletonized successfully. Less postoperative pain and easier retraction of the appendix are the advantages of this technique, and we think that this technique can be used in single port laparoscopic appendectomies.
The immediate postoperative image of the entrance point is shown in Fig. 1C. We did not observe scar tissue at the entrance point at day 20 (Fig. 1D). All procedures were done successfully. In the TLA group, we observed 1 wound infection at the periumblical region, which easily recovered with medical treatment. In the TLA group, the mean duration of operation was slightly longer than CLA group, but there was no difference in hospitalization duration.
We used a 10-mm umbilical trocar and 5-mm suprapubic trocar, endoligasure, endoclips, endobag, endoloop camera and CO2 pneumoperitoneum system in both TLA and CLA groups. In the TLA group, we used an additional needle grasper. In the CLA group, we used an additional 5-mm trocar and endoclinch. The operation cost in the TLA group was lower than the CLA group. Compared with the CLA group, the TLA technique is very cost effective.
After pneumoperitoneum was obtained, intraabdominal pathologies were easily visualized for both groups. In our study, we could easily visualize intestine, fallopian tubes, and ovaries before the appendectomy. In 1 patient, we observed a perforated Meckel's diverticulum and performed diverticulectomy with the conventional laparoscopic technique. This patient was excluded from the study.
Conversion of this technique should be performed without any hesitation, as we do not view conversion as a complication or failure. This alternative technique is very important and an obligation for emergency surgeries. In order to achieve safer visualization, the number of ports should be increased. Inserting the suprapubic trocar gives better results for retrocecal, purulent or gangrenous acute appendicitis. The suprapubic approach allows for easier dissection and is a good drainage point in cases of infection [21]. In our study, we placed 2 trocars in the TLA group and 3 trocars in the CLA group at the suprapubic region. Using this technique, we obtained easier dissection and better cosmetic results. Also, we placed drainage tubes from this hole when needed.
The decreased number of trocars may have given better cosmetic results, but there is no standardized scoring system for wound infection in order to evaluate the cosmetic results. It has been reported that there is no scar using the transparietal appendicular fixation procedure with 14-G intravenous catheter [18]. In our study, we didn't see any obvious scar tissue at the entrance point of the needle grasper at day 20, and all patients were satisfied with the cosmetic results.
As a result, TLA with the help of a needle grasper may have given better results by using fewer ports, leading to better cosmetic results and less pain. In addition, the needle grasper technique is also more cost effective than the CLA technique.




 XML Download
XML Download