

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence and prevalence rates of thyroid cancer are increasing worldwide. Moreover, the proportion of patients with papillary thyroid carcinoma (PTC) is steadily increasing [12], and PTC is 11 times more common in women than in men [3]. In the surgical treatment of PTC, when surgical techniques provideequivalent results regarding safety and completeness, patients consider cosmetic aspects. Therefore, access surgery was developed to prevent the occurrence of neck scars.
Bilateral axillo-breast approach (BABA) robotic thyroidectomy (RoT), which has been performed since 2008, is a remote access surgery technique in which four ports areplaced in the areola and axilla. BABA and other RoT approaches have achieved good oncologic outcomes and excellent cosmetic results for patients with PTC [4567].
Obesity, which is widespread and increasing, is associated with the developmentof diabetes mellitus, hypertension, cardiovascular disease, heart failure, and death from all causes [8]. In addition, obese patients pose technical and clinical challenges to the surgeons, andstudies report that high BMI is a risk factor for postoperativecomplications, specifically surgical site infection (SSI), wound dehiscence, pulmonary embolism, and renal failure [9].
Studies suggest that obesityaffectsthe surgical outcomes of thyroidectomy [101112]; however, to date, the influence of body habitus, including obesity, on thyroid robotic surgery has not been described in detail [13], and there are no studies that specifically address this association in patients undergoing BABA RoT. The aim of the present study was to evaluate the effect of body habitus on the surgical outcomes of patients undergoing BABA RoT.
METHODS
Patients
Between January 2011 and December 2012, 456 PTC patients underwent BABA RoT at Seoul National University Hospital, Seoul, Korea. BABA RoT was performed in patients with tumors smaller than 4 cm and without evidence of invasion to the trachea, esophagusor recurrent laryngeal nerve (RLN). Prophylactic ipsilateral or bilateral central lymph node dissection (CLND) was performed.This study was conducted as a retrospective analysis of prospectively collected data. All procedures were performed by three skilled surgeons who had overcome the learning curve.
All candidate patients underwent CT to evaluate the location of tumors and lymph node (LN) status following the procedure used for open thyroidectomy patients. This studywas directed at women PTC patients who had undergone BABA robotic total thyroidectomy with CLND with the aim of settling the gender ratio and standardizing surgical procedures.
This study was approved by the Institutional Review Board of Seoul National University Hospital (approval number: H-1401-120-550).
Body habitus
Body habitus was defined according to body mass index (BMI; kg/m2), body surface area (BSA; height in centimeters × weight in kg/36001/2), and neck circumference (NC; cm). According to the World Health Organization classification, patients were assigned into the following three categories: normal and underweight, BMI < 25 kg/m2; overweight, 25–29.9 kg/m2; and obese, BMI ≥ 30 kg/m2 [114]. In this study, we divided patients into 2 groups: group A, normal BMI group (BMI < 25 kg/m2); group B, high BMI group (BMI ≥ 25 kg/m2).
BSA was calculated using the Mosteller formula [15]. NC was measured horizontally at a level just below the thyroid cartilage on neck CT images, which were obtained preoperatively.
Surgical methods
The BABA RoT procedure was described previously [4]. Briefly, the procedure involves 4 stages, namely the creation of a working space, robot docking, console time (in operations using the da Vinci system console), and closure.
Patients were placed under general anesthesia and positioned in the supine position, with their neck extended. After draping, the creation of a working space was started by hydrodissection. Incisions were made bilaterally at the superomedial edge of the breast areola and the axillary folds. The flap extended from thethyroid cartilage superiorly to 2 cm below the clavicleinferiorly and from just beyond the medial border ofthe sternocleidomastoid muscle laterally using a vascular tunneler. The working space was developed using low pressure (5–6 mmHg) insufflations of CO2 gas. Four ports were inserted, and robot docking was performed.
The midline of the strap muscle was identified and separated. After visualizing the structures, the isthmus was divided with ultrasonic shears. Thyroidectomy was performed while preserving the parathyroid glands and RLN. Lesion-side central compartment dissection was performed, and the contralateral lobe was dissected in the same manner.
After complete removal of the thyroid, the operative field was irrigated with saline, and meticulous hemostasis was achieved. The midline was closed by robotic endosuturing.
Surgical outcomes
Evaluation of surgical outcomes was based on the following factors: operation time, length of hospital stay, number of retrieved central LNs, postoperative suppressed serum thyroglobulin (Tg) levels, stimulated serum Tg levels, and postoperative complications. Total operation time was subdivided into three periods as follows: working space creation time (time from hydrodissection to the placing of four trocars and CO2 gas insufflation, before robot docking), console time (the actual time required for thyroidectomy with LN dissection), and periconsole time (time required for robot docking and skin closure after console time).
To assess surgical completeness, postoperatively suppressed serum Tg levels and stimulated serum Tg levels were measured. The radioactive iodine (RAI) treatment protocol was described in detail in a previous report [16]. The first RAI treatment was performed 3 months after surgery, and the second RAI treatment was carried out approximately 9 months after surgery (6 months after the first RAI treatment). Ablation was considered successful when the stimulated Tg level at the second RAI treatment was ≤ 1.0 ng/mL in the absence of anti-Tg antibody. Serum Tg levels were assessed and neck ultrasonography was performed every 6 or 12 months during the follow-up period.
Serum total calcium, ionized calcium, phosphorus, and parathyroid hormone (PTH) levels were assessed to evaluate the development of hypoparathyroidism during hospitalization. A serum total calcium level of < 8 mg/dL with a hypocalcemic symptom during hospitalization was defined as transient hypoparathyroidism. Permanent hypoparathyroidism was defined as a serum PTH level of < 15 pg/mL with an ongoing requirement for oral calcium supplementation after 12 months [5]. In all patients, RLN function was assessed by evaluating vocal cord movement using preoperative video laryngoscopy. A return of vocal cordmovement within 6 postoperative months was diagnosed as transient RLN palsy, whereas vocal cord movement abnormalities persisting after 6 months were diagnosed as permanent RLN [5].
All patients were examined for wound complications, such as wound hematoma, seroma formation, SSI, and deformities of the areola or breast shape. Patients were routinely followed up at 2 weeks, 3 months, and 6 months postoperatively.
Statistical analyses
Statistical analysis was performed using the IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Univariate analysis was performed using the Student t-test, Mann-Whitney, chi-square, or Fisher exact tests. Statistical significance in this study was set at P ≤ 0.05. For other continuous body habitus parameters, Spearman correlation analysis was used to determine the trends of surgical outcomes with respect to BSA and NC. The adjusted odds ratios and 95% confidence intervals are reported.
RESULTS
Clinicopathologic characteristics
A total of 310 women PTC patients underwent BABA robotic total thyroidectomy with CLND with a mean age of 41.24 ± 9.6 years. Table 1 shows the demographic characteristics. The mean BMI was 22.6 ± 3.7 kg/m2; 262 patients (84.5%) were grouped in the normal BMI group, 41 patients (13.2%) in the overweight BMI group, and 7 patients (2.3%) in the obese BMI group, representing for a total of 48 patients (15.5%) in the high BMI group.A total of 185 patients (59.7%) received RAI ablation, whereas 125 patients (40.3%) did not. The mean stimulated Tg level of patients at the first RAI ablation was 0.7 ng/mL (range, <0.1–16.91 ng/mL). The percentage of patients who had stimulated Tg levels < 1.0 ng/mL and <2.0 ng/mL was 60.5% (112 of 185) and 95.1% (176 of 185), respectively. The median stimulated Tg levels of the 2 groups were 0.6 and 0.8 ng/mL. Among patients who did not receive RAI ablation, the median stimulated Tg level at 3 months postoperatively was <0.1 ng/mL (range, <0.1–8.26 ng/mL), and 95.2% (119 of 125) of patients had a suppressed Tg level of < 1.0 ng/mL. The median suppressed Tg levels of the groups A and B were 0.5 and 0.7 ng/mL, respectively. During the mean follow-up period of 34 months, none of the 310 patients experienced locoregional recurrence or metastasis.
Mean age, tumor size, tumor multifocality, tumor bilaterality, extrathyroid extension, TNM stage, and RAI ablation did not differ significantly between groups A and B (Table 2).
Surgical outcomes
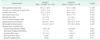
Regarding postoperative outcomes, total operation time (group A, 167.2 ± 34.9 minutes; group B, 173.7 ± 38.0 minutes; P = 0.240), creation of working space time (group A, 42.8 ± 13.0 minutes; group B, 44.5 ± 13.1 minutes; P = 0.210), console time (group A, 92.2 ± 26.3 minutes; group B, 87.8 ± 26.2 minutes; P = 0.395), and periconsole time (group A, 71.6 ± 21.1 minutes; group B, 76.4 ± 17.9 minutes; P = 0.250) showed no significant differences between the groups. There was no significant difference in the mean length of hospital stay. Regarding surgical completeness, numberof retrieved central nodes (group A, 5.3 ± 4.0; group B, 4.9 ± 3.2; P = 0.784), postoperatively suppressed serum Tg level (group A, 0.6 ng/mL [range, <0.1–10.3 ng/mL]; group B, 0.8 ng/mL [range, <0.1–12.4]; P = 0.356) and stimulated Tg level (group A, 0.5 ng/mL [range, <0.1–22.1 ng/mL]; group B, 0.7 ng/mL [<0.1–16.9 ng/mL]; P = 0.283) were not significantly different between the BMI groups.
The incidence of transient hypoparathyroidism and permanent hypoparathyroidism did not differ significantly between groups A and B. Transient RLN injury and permanent RLN injury were not significantly associated with BMI. Of 2 cases of wound complications, 1 was subareolar wound hematoma, and 1 was SSI, with no significant differences between the BMI groups (group A, 2 [0.8%]; group B, 0 [0%]; P = 0.714) (Table 3).
As shown in Table 4, surgical outcomes, number of retrieved central nodes (P = 0.566, r = 0.430), postoperatively suppressed serum Tg level (P= 0.133, r = –1.110) and stimulated Tg level (P = 0.357, r = 0.090) were not significantly associated with differences in BSA. Periconsole time (P = 0.196, r = 0.096), other operation times, surgical completeness indexeswere not significantly associated with differences in NC. The occurrence of transient hypoparathyroidism (no, 1.57 ± 0.1 m2; yes, 1.59 ± 0.12 m2; P = 0.242) and other surgical complications did correlate statistically with BSA or NC (Table 5).
DISCUSSION
The incidence and prevalence of papillary thyroid cancer is increasing worldwide, and it is more common in women than in men [123]. Studies have demonstrated the advantages of robotic surgery over traditional open surgery, such as better cosmetic outcomes, reduced postoperative nausea, and reduced pain [7101718]. Especially in thyroid surgery, robotic techniques achieve good oncologic outcomes and do not result in neck scars [56713171920].
Obesity and being overweight are major public health problems, and the rates of obesity are increasing [8]. Obesity is a known risk factor for postoperative morbidity [921]. Excess fatty tissue is more likely to become necrotic and is associated with SSI and wound complications. Obesity is considered a risk factor for BABA RoT for the following reasons: first, it can affect the creation of a working space. During the creation of working space, the surgeon generates a flap using the subcutaneous layer, which occurs after the administration of anesthesia in BABA RoT. Obesity can cause the collapse of the working space because of excessive weight and tension from the patients' thick subcutaneous flap. In addition, it may affect the incidence of wound complications such as wound hematoma, seroma formation, SSI, and deformities of the areola and breast shape. Buerba et al. [10] and Finel et al. [12] reported that obese patients had operations of greater duration and more wound complications in conventional thyroidectomy than nonobese patients. Previous work from our group showed that the morbidity of BABA RoT is similar to that of conventional surgery cases, and immediate postoperative bleeding did not occur in patients who underwent BABA RoT [6].
BSA is a measurement of the body surface that is often used in the clinical setting. Several formulas have been developed over the years, with the Mosteller formula gaining support as a standard because it is simple and easily calculated with a hand-held calculator [15]. Unlike BMI, BSA is related to height; therefore, it is associated with a greater number of anthropometric features that can affect perioperative outcomes compared with those related to BMI [22]. In the present study, BSA was associated with working space time and total operation time, whereas it was not associated with surgical outcomes or complications in female patients. NC is a valid marker of obesity that correlates well with other anthropometric measurements; it is an accurate indicator of upper-body fat distribution, which is closely correlated with visceral adiposity [2324]. The amount of subcutaneous fat in the upper body may be associated with the complications of surgery. In the present study, NC was associated with working space time, whereas it showed no correlation with surgical outcomes or complications in female patients.
Serum Tg level is a useful indicator of residual disease during the postoperative follow-up of patients who undergo total thyroidectomy, and it is an indicator of surgical completeness [25]. Although the levels may be measured while thyroid-stimulating hormone (TSH) is suppressed, the test is more sensitive when TSH is stimulated [26]. Stimulated Tg level is directly related to the amount of residual thyroid tissue [2728], and it is a useful method to predict persistent or recurrent disease by measuring the thyroid bed 131I uptake after first RAI ablation [27]. A previous study showed that 48.3% of 729 patients with low-risk thyroid carcinoma had a stimulated Tg level <1 ng/mL [28]. This study showed good results compared with those of conventional total thyroidectomy, as reported previously.
A previous study has shown that transient hypoparathyroidism after thyroidectomy is a common occurrence (1.6%–50% of interventions) [29], and the rate of permanent hypoparathyroidism after thyroidectomy is reported to range from 0% to 1.3% [30]. The incidence of this complication in our study was not statistically significantly different between the groups and did not significantly depart from the rates reported in the literature. Permanent RLN palsy after conventional total thyroidectomy is reported to occur in 0%–1.3% of cases. In this study, we found that 2 cases (0.8%) had permanent RLN, although the incidence of RLN has been reported not to be statistically significant between BMI groups [25].
The present study has several limitations. Firstly, the data was retrospectively analyzed, which could have resulted in bias inthe selection of BABA RoT patients. Secondly, the low number of obese patents analyzed limited the accuracy of the statistical analysis. Despite these limitations, the present study indicates that BABA RoT offers surgical completeness and oncological safety in patients with different body habitus and may be a good alternative operative method for PTC patients.




 XML Download
XML Download