

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Jejunal diverticulosis is a very rare clinical entity, and is identified in 0.02% to 0.42% of standard radiological studies. In autopsy series, the incidence has ranged from 0.06% to 4.6% [1]. The majority of patients with jejunal diverticulosis are asymptomatic [2]. Chronic abdominal symptoms (abdominal pain, nausea and vomiting, flatulence, diarrhea, etc.) have been described, as have more acute symptoms, presenting with major complications including diverticulitis, gastrointestinal hemorrhage, intestinal obstruction, and acute perforation. We report a case of uncomplicated jejunal diverticulosis with pneumoperitoneum.
CASE REPORT
A 55-year-old woman with aggravated periumbilical abdominal pain and pneumoperitoneum on plain chest and abdominal films was admitted urgently from a local clinic (Fig. 1). She had suffered for approximately 10 years with intermittent left upper quadrant abdominal pain, and her past medical history included hypertension and a total hysterectomy owing to menorrhea. Her abdomen was slightly distended but soft.
She was hemodynamically stable with soft, minimal tenderness on the left upper quadrant of the abdomen, but she had no rebound tenderness. Her hemoglobin level was 12.8 g/dL, white blood cell count was 12,400 cells/µL, and CRP level was 0.08 mg/dL.
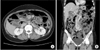
Abdominal CT showed one clockwise rotation of the superior mesenteric artery and superior mesenteric vein root. There was no evidence of bowel dilatation or vascular impairment, suggestive of impending midgut volvulus, and there were small (less than 5 mm in size) diverticula in the mid jejunum, suggestive of jejunal diverticulosis (Fig. 2).
Because of the longstanding clinical symptoms and pneumoperitoneum on the plain chest film, a laparotomy was suggested to the patient.
The surgery confirmed the presence of small bowel torsion and jejunal diverticulosis. Over 30 small bowel diverticula of various sizes (maximum 4 cm) were noted on the mesenteric side of the proximal jejunum. The affected segment of the jejunum was approximately 180 cm (20–200 cm below the ligament of Treitz), but on further investigation no perforation site was found. After derotation, we did not resect any diverticulum since the affected segment was too long and did not appear to have any complications (Fig. 3).
No postoperative complications were observed, and the patient made a full recovery. She was discharged 7 days after the operation.
DISCUSSION
Small bowel diverticulosis was first described by Baillie and von Soemmerring [3] in 1794 and Cooper [4] first described Jejunal diverticulosis in 1807.
The prevalence of small intestinal diverticula on autopsy ranges from 0.06% to 4.6% [1]. The prevalence increases with age, peaking at the sixth and seventh decades. A higher incidence had been reported in men than in women [5], but more recent data suggests a possible reversal in the sex distribution [6].
Small bowel diverticulosis was previously considered as incidental anomalies, but is now thought to be acquired [57]. Small bowel diverticulosis is thin-walled sacculations that, in contrast to Meckel diverticula, consist only of mucosa, submucosa, and occasionally a thin layer of serosa without muscle [8]. These false diverticula are acquired herniations of mucosa, through gaps in the muscle layers along pathways of the visceral vessels at the site of entry of the vasa recta, commonly found on the mesenteric border of the jejunum. The pathogenesis of small-bowel diverticula is unclear, but they probably occur because of motor dysfunction of the smooth muscle or dysfunction the myenteric plexus in the small bowel [7]. The sizes of these diverticula vary from a few millimeters (mm) to greater than 10 cm, and the predominance of diverticula in the jejunum is attributed to the large diameter of the penetrating jejunal arteries [25]. Coexistent diverticulosis is found in the colon in 20%–70%, in the duodenum in 10%–40%, and in the esophagus and stomach in 2% of patients [68].
The clinical presentations are variable and include vague and chronic epigastric or periumbilical abdominal pain of varying severity, with a bloating sensation after food intake. Usually the disorder is clinically silent until it presents with complications—the relative clinical rarity and varied presentation of this disease may delay and impair diagnosis. As a result, diagnosis is frequently made incidentally either by radiographic examination or upon laparotomy owing to complications.
The reported complications of jejuno-ileal diverticulosis occur in 10%–30% of patients and include chronic abdominal pain, malabsorption, hemorrhage, diverticulitis, obstruction, abscesses in the mesentery, and perforation. The most common acute complication of the jejuno-ileal diverticula is diverticulitis with or without perforation, which occurs in 2.3%–6.4% of cases [28], and has a mortality rate as high as 24% [9].
This may be associated with obscure gastrointestinal bleeding or bacterial overgrowth and may, on occasion, become impacted with ingested food and inflamed, and present with acute abdominal pain.
The diagnosis of complicated or uncomplicated jejunal diverticulosis is seldom made before exploratory laparotomy or diagnostic laparoscopy. Various radiographic techniques such as ultrasound, computed tomography, endoscopy, capsule endoscopy, intraoperative endoscopy, deep enteroscopy (with single or double-balloon enteroscopy or spirus enteroscopy), laparoscopy, radio-tagged erythrocyte bleeding scans, and selective mesenteric arteriography, have been recently used for detection with increasing success. However, many lesions can escape diagnosis. If the diverticular ostium is large, the diverticula can rapidly empty and not be visible. Small diverticula may not retain contrast medium as well, or may not be filled with contrast medium at all. Laparotomy remains the gold standard for definite diagnosis of asymptomatic and complicated diverticula.
Pneumoperitoneum is commonly found after perforation of diverticula. However, pneumoperitoneum without perforation or concomitant signs of peritonitis is rarely found. This spontaneous, usually asymptomatic pneumoperitoneum has been hypothesized to be the result of a rapidly closed leaking diverticulum, or of the transmural passage of air through a thin-walled diverticulum. Pneumoperitoneum has been associated with the presence of pneumatosis cystoides intestinalis or subserosal dissection of air around the bowel or surrounding structures.
Conservative treatment of uncomplicated patients involves nonspecific measures such as high-protein and low-residue diet, vitamin supplementation, antispasmodics, antidiarrheal agents, antacids, and analgesics [210], and success rates of 46%–75% have been reported [2]. Most investigators who found ileal diverticula incidentally at laparotomy did not necessarily perform resection [10]. However, some authors favored surgical intervention, and reported good results for resections performed on patients with chronic pain or malabsorption [8]. Multiple jejunal diverticula have prompted resection of as much as 75 cm of the small bowel, offering symptom relief; however, recurrence of symptoms is more common in these patients compared with the nonsymptomatic patients (53% vs. 17%) [2]. Resection of the affected area with primary jejunojejunal anastomosis is the surgical management of choice in the presence of perforated jejunal diverticular disease, hemorrhage, or abscess formation after failure of a short course of bowel rest and antibiotics. However, the surgeon should avoid, if possible, extensive bowel resections to prevent short bowel syndrome.
In conclusion, jejunal diverticula are rare, but they should not be regarded as insignificant. For uncomplicated patients with symptoms such as chronic abdominal pain or malabsorption related to jejuno-ileal diverticulosis, conservative management is the initial treatment option. However, when the patient remains unresponsive to conservative treatment or when complications occur, surgical resection is the preferred option.


 XML Download
XML Download