

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ischemic heart disease (IHD) is prevalent in patients with abdominal aortic aneurysm (AAA) and is known to be a major cause of early and late death following elective AAA repair. According to the endovascular aneurysm repair (EVAR)-1 trial [1], IHD was the primary cause of death during the follow-up period after AAA repair (27.2% of patients after EVAR and 22.5% of patients after open surgical repair [OSR]). The reported prevalence of IHD in AAA patients varies widely among studies due to racial difference of the study population and nonstandardized, different diagnostic criteria of IHD.
Hertzer et al. [2]'s report has been frequently cited as a standard reference regarding the prevalence of concomitant coronary artery disease (CAD) in patient with AAA. There has been no report from Korea regarding the prevalence of concomitant IHD and risk factors for postoperative acute myocardial infarction (PAMI) after elective AAA repair.
Management strategy of the concurrent IHD in patients with AAA has been on a debate. Some authors [3] reported that coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) prior to elective vascular surgery may reduce the risk of perioperative cardiac events and improve long-term survival. However, other authors [45] reported that there was no benefit of prophylactic coronary revascularization over medical treatment before major vascular surgery on perioperative or long-term results.
We aimed to determine the prevalence of concomitant IHD in Koreans patients with AAA and to see the risk factor for an early postoperative myocardial infarction after elective AAA repair.
METHODS
A retrospective review of 765 patients who underwent AAA repair in a single institution from September 2003 through December 2014 was performed of which 602 patients (male, 87.7%; mean age, 70 ± 8 years) undergoing elective repair of infra- or juxtarenal AAA (373 OSRs and 229 EVARs) were enrolled in this study. Excluded were patients who had repair of ruptured AAA (n = 62), symptomatic AAA (n = 18), Marfan syndrome (n = 16), infected AAA (n = 36), type IV thoracoabdominal or suprarenal AAA (n = 17), and redo aortic surgery following prior OSR or EVAR (n = 14).
Prior to elective AAA repair with either OSR or EVAR, work up for IHD was carried out following a standardized algorithm. We evaluated for a past history of cardiac events, cardiac symptoms, hospitalization due to acute chest pain with abnormal ECG changes, coronary interventions, and cardiac related medications then consulted with a cardiologist before elective AAA repair.
Protocol for preoperative cardiac evaluation prior to elective AAA repair is shown in Fig. 1. Until 2009, we performed routine preoperative measurements of cardiac enzymes (creatine kinase-myoglobin [CK-MB], troponin-I) and N-terminal pro-brain natriuretic peptide, 12-lead ECG, screening echocardiography, and TI-201 adenosine single-photon emission computerized tomography (SPECT). After 2009, assessment of cardiac stress function was selectively performed according to guidelines of the American College of Cardiology/American Heart Association [6] using TI-201 adenosine SPECT (n = 234, 38.9%) or adenosine stress myocardial perfusion CT (n = 100, 16.6%) or dobutamine stress echocardiography (n = 50, 8.3%).
Preoperative coronary artery angiography (CAG) was performed based on the recommendation of the consultant cardiologist in cases of left main coronary artery stenosis >50% or other coronary artery stenosis >70% with perfusion defect on preoperative adenosine stress myocardial perfusion CT; functional class III or IV (Canadian Cardiovascular Society Functional Classification of Angina Pectoris) with significant coronary artery stenosis; left ventricle ejection fraction <40% with significant coronary artery stenosis or perfusion defect; moderate to severe ischemia in ≥2/16 segments with new regional wall motion abnormality (RWMA) or ≥5/16 segments with RWMA by dobutamine stress echocardiography; or myocardium ischemia >10% on TI-201 adenosine SPECT.
Postoperatviely, cardiac troponin I (cTn-I) was routinely measured for all patients. PAMI was defined as elevated cTn-I level >5 times the upper normal level (>3.9 ng/mL) or elevated cTn-I level in conjunction with one or more of the following conditions: presence of ischemic cardiac symptoms; ECG finding of new significant ST or T wave change, new left bundle branch block, or pathologic Q wave; new RWMA on cardiac imaging study; or coronary lesion on CAG [7].
Based on the history of IHD and results of preoperative cardiac evaluation, we classified AAA patients into 3 groups: control group (patients with no evidence of IHD); group I (patients with past history or positive findings of IHD on preoperative evaluation who were medically treated without any invasive coronary intervention); and group II (patients who underwent coronary revascularization either PCI or CABG).
We investigated the frequency of early (<30 days) PAMI and cardiac mortality in each group and also according to the type of AAA repair. To determine characteristics of patients who developed PAMI, we conducted a univariable and multivariable analysis using Mann-Whitney, Fisher exact, chi-square test and multiple logistic regression analysis.
Statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Continuous variables were described as mean ± standard deviation and categorical variables were expressed as number and percentage of subjects. Each variable was tested for normality before statistical analysis. Age-adjusted logistic regression analysis was conducted to evaluate differences in the frequencies of PAMI between the groups and according to the type of AAA repair. All tests were two-sided, and statistical significance was defined as P < 0.05.
RESULTS
Of 602 elective AAA repairs (373, 62% OSR and 229, 38% EVAR), patients (mean age, 70 ± 8 years; male, 87%) were categorized into control (398 patients, 66%), group I (73 patients, 12%), and group II groups (131 patients, 22%). In group II patients, 18 patients who underwent coronary artery revascularization (CAR) before AAA repair on the basis of preoperative cardiac risk evaluation were included. Table 1 shows a comparison of patient characteristics between the groups. Patients who underwent OSR in the control group were significantly younger than other groups (control, 67.5 years vs. group I, 70.3 years vs. group II, 72.2 years, P < 0.002). There was no difference in comorbidities or atherosclerotic risk factors except frequency of IHD between groups. As expected, cardiovascular disease-related medication use was more frequent in groups I and II patients compared to control group.
In group II patients, the median time interval between CAR and an elective AAA repair was 45.1 months (range, 1–205 months) after PCI (n = 81) and 45.2 months (range, 0–228 months) after CABG (n = 50).
In early postoperative period after elective AAA repair, we observed elevated serum cTn-I level (>0.78 ng/mL) in 40 patients (6.6%) (36 OSR, 90% vs. 4 EVAR, 10%, P < 0.001). Among the 40 patients, 23 patients (3.8%) met diagnostic criteria for PAMI whereas the remaining 17 patients were considered to have stress-induced cardiomyopathy or subclinical myocardial infarction.
Table 2 shows the frequencies of PAMI and mortality after AAA repairs. Frequency of an early PAMI was significantly higher in the patients undergoing OSR compared to EVAR (5.4% vs. 1.3%, P = 0.012). In subgroup analysis, we found that PAMI developed more frequently in patients with IHD (groups I and II) after OSR compared to the control group. This difference between groups did not apply in the EVAR groups (Fig. 2). Ageadjusted PAMI rate was significantly higher in group I compared to the control group (18.0% vs. 2.1%; odds ratio, 9.03; 95% confidence interval, 2.86–28.57; P = 0.001). Considering patient group and AAA treatment modality together, OSR in group I patients showed the highest rate of PAMI. In the comparison of PAMI rates after OSR between groups I and II, there shows a trend towards higher PAMI rate in group I compared to group II (18.0% vs. 7.1%, P = 0.057) (Fig. 2) but this did not reach statistical significance.
There were 3 postoperative deaths (0.5%) including 2 cardiac related following OSR and 1 due to sepsis from spontaneous gall bladder rupture after EVAR (Table 2).
Through preoperative cardiac evaluation, 55 patients (9.1%) undertook catheter-based CAG prior to elective AAA repair. Among these patients, 36 patients underwent an elective AAA repairs (26 OSRs, 10 EVARs) without coronary revascularization whereas 18 patients (32.7%) underwent CAR (10 PCIs and 8 CABGs) prior to AAA repair (12 OSRs, 6 EVARs). In one patient with severe CAD and large diameter AAA, OSR of AAA and CABG were synchronously performed.
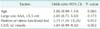
On an univariable risk factor analysis for development of PAMI, PAMI developed more frequently in patients with older age group, larger AAA diameter, multivessel CAD (stenosis ≥50% affecting 2 coronary arteries), involvement of the left main coronary artery, and positive functional stress test (Table 3). On the logistic regression analysis, a positive result on a preoperative functional stress test was the only significant risk factor for PAMI after an elective AAA repair either OSR or EVAR (Table 4).
DISCUSSION
IHD is known to frequently coexist in patients with AAA [28]. The most common cause of perioperative death following elective AAA repair is also cardiac related death [19]. In this retrospective study, we observed the prevalence of concomitant IHD in Korean AAA patients was approximately 34%. This is in line with reports from other Asian countries that reported prevalence of IHD in AAA patients ranging from 27% to 65% [101112]. This wide range of prevalence in these reports may be attributable to variable diagnostic criteria and diagnostic tools used to diagnose IHD.
After elective repair of infra- or juxtarenal AAA, we report an overall 3.8% frequency of PAMI (OSR, 5.4% vs. EVAR, 1.3%, P = 0.012) and 0.5% rate for surgical mortality (OSR, 0.5% vs. EVAR, 0.4%, P = 1.000). We found that PAMI developed more frequently in patients with IHD (groups I and II) compared to control group (control, 2.1%; group I, 18.0%; group II, 7.1%, P < 0.001). Unlike the OSR group, coexisting IHD did not show a significant adverse impact on the development of PAMI in EVAR group.
Among randomized controlled trials (RCTs), EVAR-1 [1], DREAM (Dutch randomized endovascular aneurysm management) trial [13], and OPEN (open versus endovascular repair) trial [14] reported higher surgical mortality following OSR compared to EVAR but did not report frequency of PAMI. In the anevrysme de l'aorte abdominale, chirurgie versus endoprothese (ACE) trial [15], frequency of PAMI after OSR and EVAR was the same (0.6% vs. 0.6%), and there was no statistical difference in mortality after OSR and EVAR (0.6% vs. 1.3%, P = 1.000). However, the definition of acute myocartial infarction (AMI) in the ACE trial was not clearly described. Unlike other randomized prospective trials, the ACE trial only included low or intermediate surgical risk patients.
A report by Hertzer et al. [2] from the Cleveland Clinic has been cited as a standard reference regarding the prevalence of CAD in patients undergoing elective AAA repair. They reported a 94% rate of CAD in 263 AAA patients by routinely performed catheter-based CAG prior to an elective AAA repair. Many previous studies have described the importance of cardiac evaluation before elective AAA repair [16]. Contrary to them, the benefit of routine preoperative CAG and CAR before elective AAA repair has been disputed. McFalls et al. [4] reported no survival benefit of CAR before elective major vascular surgery in long-term postoperative follow up. The DECREASE-V pilot study [5] also showed that prophylactic CAR in patients with 2,3-vessel or left main CAD did not improve outcomes at 30-days and 1 year after major arterial surgery. In the present study, we observed that AAA patients with concomitant IHD showed more frequent PAMI after elective OSR of AAAs but not in EVAR group. More frequent occurrence of PAMI did not result in higher surgical mortality.
Currently, the development of more sensitive and specific cardiac biomarkers has led to make the diagnosis of acute myocardial infarction easier [7]. Unlike classic AMI in nonsurgical patients, diagnosis of PAMI can be difficult to make because the characteristic chest pain or ECG findings may be obscured in the early postoperative period [17] and CK-MB fraction elevation may be inconsistent [18]. Cardiac troponins (cTn) are highly sensitive and specific biomarkers for myocardial damage that have been used for diagnosis of PAMI [192021]. Some authors introduced the term "clinically relevant myocartial infarction (MI)" as a new definition [22]. They propose that AMI with low or no subsequent mortality or heart failure may be misinterpreted as true AMI. Therefore, they recommend a higher threshold level of cardiac biomarkers for the diagnosis of true PAMI. According to the third universal definition of AMI [7], periprocedural MI was defined as cTn-I level >5 times of the upper normal limit.
There are two distinct mechanisms for PAMI: acute coronary syndrome (type 1) and prolonged myocardial oxygen supplydemand imbalance (type 2) [23]. Type 1 AMI occurs by spontaneous rupture of an unstable or vulnerable plaque, leading to acute coronary thrombosis, myocardial ischemia, and infarction. Type 2 AMI occurs when myocardial oxygen demand is greater than its supply due to increased myocardial oxygen, decreased subendocardial oxygen supply, or both. Type 2 AMI ranges from a silent MI with minor elevation of cardiac troponin level to a prolonged, overt ischemia with marked troponin elevation [23].
In the present study, we found only one symptomatic PAMI after elective AAA repairs while all other patients asymptomatic but showing ST-depression (n = 10) or elevated serum troponin level >5 times the upper limit of normal (n = 20). For treatment of 23 patients with PAMI, 2 patients (8.7%) required CAR (1 PCI and 1 CABG) during the early postoperative period while the others were treated with medical management. Some authors have reported that patients with perioperative subclinical MI with an elevated troponin level exhibit decreased long-term survival on follow up observation [21242526].
In the present study, patients with coexistent IHD (groups I and II) developed PAMI at significantly higher rates compared to the control group after OSR but this finding was not shown in the EVAR group. On a subgroup analysis, group I patients seems to be associated with higher rate of PAMI after OSR than group II patients, however, this did not reach statistical significance (18% vs . 7%, P = 0.057). Among the group II patients, 18 patients who underwent CAR before AAA repairs on the basis of preoperative cardiac risk evaluation were included.
We experienced operative mortality rates of 0.5% after OSR and 0.4% after EVAR. The death of 2 patients after OSR was due to PAMI and 1 postoperative death after EVAR was due to septic shock secondary to spontaneous rupture of gallbladder in the early postoperative period. Though there was a difference in PAMI occurrence between OSR and EVAR, we did not find a significant difference in operative mortality between the OSR and EVAR groups. Compared to Western series, we have experienced lower rate of PAMI and early postoperative cardiac mortality. It might be attributable to the different behavior of CAD in Korean patients from the patients in the western countries.
Through the preoperative cardiac evaluation, we decided 55 patients (9.1%) are requiring catheter-based CAG. Among these 55 patients, coronary revascularization (10 PCIs and 8 CABGs) was performed in 18 patients (32.7%) prior to their AAA repair and 1 patient underwent combined OSR of AAA and CABG. In this small group of patients who underwent catheter-based CAG prior to AAA repair, we found that the frequency of PAMI was lower in patients who underwent coronary revascularization before AAA repair compared to patients who proceeded to AAA repair without coronary revascularization, but the difference did not reach statistical significance (2 of 18 [11.1%] vs 5 of 36 [13.9%], P = 0.775). Considering that patients who underwent CAR had more severe CAD, these results can be translated as a beneficial effect of preliminary CAR in selective group of AAA patients with severe CAD.
On an univariable risk factor analysis for PAMI, we found that PAMI developed more frequently in patients with older age group, larger AAA diameter, multi-vessel CAD (stenosis ≥50% affecting 2 coronary arteries), left main coronary disease, and positive functional stress test. And multivariable analysis for PAMI, positive stress test was the only significant predictor of PAMI.
The current study is limited by its retrospective study design and change in preoperative cardiac evaluation protocol during the middle of the study period. Also, although a higher threshold of diagnostic criteria for PAMI was used, stress-induced cardiomyopathy or pulmonary embolism could have caused elevated cardiac biomarkers and could be a confounder in the diagnosis of PAMI. As limitations of our study, group II patients who underwent prior coronary artery reconstruction may have variable characteristics due to uncertainty of the patency of the reconstructed coronary arteries at the time of AAA repair in addition to the inherent limitations of retrospective study design.
In summary, we found concomitant IHD in 34% of Korean patients undergoing elective AAA repair by preplanned preoperative cardiac risk evaluations of AAA patients. The risk of PAMI was significantly higher in patients with IHD in OSR group, especially in the patients who had IHD on medical treatment without coronary intervention, compared to the Control group or EVAR group. Although the risk of PAMI was significantly higher for patients with IHD than in control group, there was no significant difference in surgical mortality between the groups after elective repair of AAA either EVAR or OSR.
In conclusion, presence of IHD was a predictor of PAMI in patients undergoing OSR of AAA. However, this finding was not true for EVAR group. Preoperative cardiac evaluation, particularly functional stress test can predict an occurrence of PAMI after elective AAA repair. However, cardiac death was uncommon in Korean patients who underwent elective AAA repair.





 XML Download
XML Download