

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatoduodenectomy (PD) is the standard surgery for malignant diseases and severe injuries involving the periampullary region. The safety of this procedure has been much improved recently, with a 0%-5% mortality rate in the most high-volume center [123]. However, PD is still associated with a significant incidence of postoperative morbidities, such as pancreatic fistulas, delayed gastric emptying, and hemorrhaging [4].
Among three anastomoses for the continuity of the remnant pancreas, bile duct, and duodenum, pancreaticojejunostomy (PJ), which is commonly favored by surgeons, remains the "Achilles heel" of PD because pancreatic fluid leakage from the procedure is potentially lethal morbidity even for the most experienced surgeons. Pancreatic fistulas still occur at a frequency of 5% to 30% [56789101112]. Various methods, such as using stents, applying fibrin glue, using duct occlusion, and modifying the different PJ techniques, have been devised to avoid leakage from PJ; the effects of these efforts on postoperative pancreatic fistulas (POPFs) are controversial [13]. Furthermore, it is still debatable whether different types of PJ actually reduce the leakage rate.
The concept of the POPF, recently defined by the International Study Group of Pancreatic Fistula (ISGPF), may be useful in comparing the efficacy of various PJ techniques, as the rate of leakage varies according to the different definitions pancreatic fistula [14].
Langrehr et al. [15] developed a simple "mattress suture technique" that may avoid the tangential shear forces that are unavoidable in a conventional duct-to-mucosa PJ (DM) during the tightening of the knots. In their technique, the sutures penetrate straight through the pancreatic remnant to avoid tearing the parenchyma by the tangential shear force. Compared with the outcomes of conventional PJ, the authors reported a trend toward fewer reoperations by using this technique, but the complication rates and the lengths of the hospital stays were similar. However, their new technique appeared to cause mucosal protrusion and tearing of the anterior jejunal wall. Thus, we modified the original "mattress suture technique" by inverting the seromuscular layer of the jejunal posterior and anterior walls. We call this modification the "inverted mattress PJ (IM)". In this study, we present the IM technique and compare this modified technique to the conventional DM technique, focusing in particular on POPF as defined by ISGPF.
METHODS
From June 2003 to December 2010, 186 consecutive patients underwent a PD by a single surgeon. From June 2003 to June 2007, a conventional duct-to-mucosa PJ was utilized for 52 of the patients (the DM group), whereas the inverted mattress PJ was utilized for the other 134 patients (the IM group) beginning in June 2007. Twenty-five PD cases performed before June 2003 were excluded to remove the effect of the learning curve on the leakage from a PJ.
The clinical features and surgical outcomes of the IM group were compared with those of the DM group, which was used as a historical control. To determine the effects of the IM technique on pancreatic fistulas objectively, we adopted the definition of POPF used by the ISGPF [12]. The clinicopathological features and surgical outcomes, including the rate of POPF, duration of the hospital stay, morbidities, and 30-day or in-hospital mortality, were compared between the 2 groups. Chi-square and t-tests were utilized for the statistical analyses.
Surgical techniques
The pylorus-preserving PD was most commonly employed. Lymph node dissection around the common hepatic artery and the hepatoduodenal ligament was performed routinely for malignant diseases. After the specimen was removed, various types of surgical procedures for gastrointestinal continuity, such as duodenojejunostomy and hepaticojejunostomy, were utilized for each specific case; however, only the conventional duct-to-mucosa PJ or the IM were performed for the PJ of the former 52 patient (the DM group) and the subsequent 134 patients (the IM group).
An external stent was inserted routinely into the pancreatic duct, but no patients received prophylactic octreotide to prevent POPF. At the end of the procedure, 2 closed-suction drains were placed near the sites of the hepaticojejunostomy and the PJ.
We modified the original "mattress suture technique" illustrated by Langrehr et al. [15] by inverting the seromuscular layer of the jejunal posterior and anterior walls with 5 to 6 U-shaped mattress sutures. The following are the details of the inverted mattress PJ.
Inverted mattress technique for PJ
Antimesenteric border of the proximal jejunum measuring the same size as the pancreatic cut surface was longitudinally opened. Three-to-four U-shaped mattress sutures (4-0 Prolene, Ethicon Inc., Somerville, NJ, USA) were placed starting at the serosa of the posterior jejunal wall and going out-in through the full thickness of the jejunum. Then, inverted seromuscular stitches were placed going in-out (Fig. 1A). These sutures penetrated the pancreatic remnant in a straight manner. (Fig. 1B). The seromuscular layer of the anterior jejunal wall was inverted by the transpancreatic U-shaped sutures going out-in followed by a full thickness stitch in the anterior jejunal wall going in-out, thereby invaginating the pancreatic remnant into the lumen of the jejunum (Fig. 1C).
A U-shaped suture was placed in a corner of the jejunum starting at the serosa of a jejunal wall and going out-in through the full thickness of the jejunum. Then, inverted seromuscular stitch was placed going in-out. The suture penetrated an end of pancreas stump in a straight manner then seromuscular layer of the other jejunal wall was inverted by the transpancreatic U-shaped suture going out-in followed by a full thickness stitch in the jejunal wall going in-out. Finally, in the same way, a U-shaped suture at the other corner of jejunum fixed the other end of pancreas.
The 5-6 U-shaped sutures, including the sutures at both corners of the jejunum, were pulled over using adequate tension (Fig. 1D) and tied at the anterior wall and at both corners of the jejunum, thereby enclosing the jejunal opening around the remnant pancreas.
RESULTS
Clinicopathological features of the patients
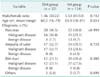
The mean patient age in the DM and IM groups were 60.3 (range, 16-78 years) and 63.9 years (range, 18-81 years), respectively. The male to female ratio did not differ between the DM and IM groups (1.36 vs. 1.53). The diseases included 158 malignancies and 28 benign diseases. The indications of PD did not differ between the 2 groups (Table 1).
The histopathologic diagnoses included adenocarcinoma of the pancreas, distal bile duct carcinoma, and carcinoma of the papilla, among other diagnoses. The DM group included 16 pancreatic head adenocarcinomas, 12 distal bile duct carcinomas, 17 ampullary carcinomas, and other diagnoses. The IM group included 36 pancreatic head adenocarcinomas, 8 other tumors of the pancreas, 36 distal bile duct carcinomas, 31 ampullary carcinomas, and other diagnoses (Table 2).
Comparison of the surgical outcomes between the conventional DM and IM groups
The median operative time was 573 minutes (range, 407-806 minutes) for the DM group and 459 minutes (range, 266-842 minutes) for the IM group (P < 0.001). The median length of the hospital stay was 28 days (range, 14-133 days) for the DM group and 24 days (range, 11-186 days) for the IM group. Pancreatic fistulas defined as grades A to C occurred in 51.9% of the patients (27/52) in the DM group and in 38.8% of the patients (52/134) in the IM group. Incidence of POPF in our results was much higher than that in reported series. Especially, grade A pancreatic fistula occurred much frequently in both group. This may be partly because we measured the amylase level in the drain fluid repeatedly for all patients regardless of clinical condition until this level declined.
Grade B pancreatic fistulas occurred in 11.5% of the patients (6/52) in the DM group and in 9.7% of the patients (13/134) in the IM group. POPFs of grades B and C, which have a clinically significant impact on patient outcomes after surgery, occurred less frequently in the IM group (17.3% vs. 9.7%, P = 0.20) compared with the DM group, but the difference did not reach statistical significance. Importantly, compared to 5.8% of grade C pancreatic fistulas in the DM group, no grade C pancreatic fistulas occurred among the patients who underwent IM (IM group, P = 0.020). Hemorrhaging from a gastroduodenal artery pseudoaneurysm occurred in 1.9% of the patients (1/52) in the DM group, whereas no patients in the IM group developed gastroduodenal artery pseudoaneurysms (P = 0.280). Mortality occurred in 1.9% of the patients (1/52) in the DM group and in 1.5% of the patients (2/134) in the IM group. For the 3 mortalities, the causes of death were sudden cardiac arrests secondary to preexisting arrhythmias in the early period after surgery in two cases and central vein catheter-related Candida sepsis in one case. POPF was unrelated to these three mortalities in this study (Table 3).
DISCUSSION
The leakage of pancreatic fluid from pancreaticoenterostomy is common and is the most serious because it is associated with subsequent lethal complications, such as abscesses, sepsis, and bleeding from eroded vessels, which can cause death. Various authors report the incidence of pancreatic fistulas as 5% to 30% [56789101112]. The difference in their findings may be due to the inconsistent definition of pancreatic fistula, which makes it difficult to compare different PJs. Thus, adoption of the ISGPF's POPF definition may be appropriate for the study to identify the factors influencing the incidence of pancreatic fistulas.
The risk factors of POPF are known to include the type of pancreaticoenteric anastomosis, texture of the pancreas, duration of the operation, intraoperative blood loss, ischemia of the jejunal/pancreatic cut ends, patient-related factors, and surgeon volume. Among these factors, the type of pancreaticoenteric anastomosis may be the most important because it can be targeted and modified [161718].
Among the many different types of pancreaticoenterostomies, most surgeons commonly favor the PJ. The PJ technique can be grouped with either duct-to-mucosa or invagination PJs. In either technique, if the sutures hold thin pancreatic tissue, the tangential shear forces formed by the suture material can easily cut into the pancreatic tissue during the tightening of the knots. To avoid this problem, Langrehr et al. [15] and Kleespies et al. [19] reported the effects of the transpancreatic U-suture technique, which is free from tangential tension and shear forces.
Langrehr et al. [15] reported using the mattress PJ technique with transpancreatic U-sutures with invagination. In this anastomosis, the surgeon pulls the jejunal loop over the pancreatic remnant, and then the sutures are led straight through the pancreatic remnant, thereby avoiding the tangential shear forces that occur during the tightening of the knot. According to their report, although total surgical complications (31.6%) and pancreatic leakage (3.5%) did not significantly differ between the 2 techniques, they concluded that this technique is faster, simple, safe, and suitable for training schedules in pancreatic surgery because the mattress technique is not as technically demanding.
Similar to this technique, Kleespies et al. [19] developed a new transpancreatic U-suture technique that was combined with a duct-to-mucosa anastomosis. They called their method the "Blumgart anastomosis (BA)" and compared it with the modified Cattell-Warren anastomosis (CWA). The authors reported a shorter duration of operation, a lower pancreatic leakage rate, and fewer surgical complications utilizing the BA compared with the CWA. They concluded that BA was faster, safer, and associated with a reduced rate of pancreatic fistula. Grobmyer et al. [20] also recently reported a 6.9% rate of clinically significant pancreatic fistulas (POPF grades B and C) using the U-suture technique developed by Blumgart.
When performing the transpancreatic U-suture technique described by Langrehr et al. [15], there are 2 potential problems. First, jejunal mucosa could protrude between the posterior jejunal wall and the pancreatic parenchyma. Second, anterior sutures between the anterior jejunal wall and the pancreatic parenchyma may be weak because the stitches include only the seromuscular layer of the anterior jejunal wall. Thus, we modified the mattress PJ technique reported by Langrehr et al. [15] to invert the seromuscular layer of the posterior jejunal wall before penetrating the pancreas and to include the full layer of the anterior jejunal wall's inverted seromuscular layer in the suture after penetrating the pancreatic parenchyma. We call this modified technique the "Inverted Mattress Pancreaticojejunostomy". This procedure is illustrated in Fig. 1.
The results of this technique were compared to a historic control using a before-after study design. To remove the effects of the surgeon factor and learning curve on the frequency of PJ leakage, we selected cases that were performed by a single surgeon, excluding the early cases performed before the period of this study.
In detail, the average operative time was shorter in the inverted mattress group and showed statistical significance (P < 0.020). The hospital stay duration was shorter in the inverted mattress group, although it did not reach statistical significance (P = 0.350). The pancreatic fistula rate dropped after the adoption of the inverted mattress technique. Of particular importance in our study is that the patients who underwent a modified inverted mattress PJ had no incidence of grade C pancreatic fistula (P = 0.020), which causes us to favor using the IM technique after PD.
In our study, using the inverted mattress PJ, the incidence of all pancreatic fistulas from grades A to C was 38.8%. Although this incidence appears to be greater compared with other studies, the rate of clinically significant grades B and C pancreatic fistulas was 9.7% and 0%, respectively. This rate is similar to the results of recent reports utilizing the ISGPF definition and grading system, which reported 7% to 15% clinically significant grades B and C pancreatic fistulas [2122232425].
A hard pancreatic remnant with dilated pancreatic ducts is technically easier and safer for anastomosis, and results in a lower rate of pancreatic fistula compared with a soft pancreatic remnant that is functionally normal and secretes a large amount of pancreatic fluid. Therefore, patients with pancreatic diseases, such as chronic pancreatitis and pancreatic cancer, have been reported to have fewer incidences of postoperative leakage [1319252627].
In our study, the frequency of pancreatic diseases, such as pancreatic cancer and chronic pancreatitis, was lower (38.8%) compared with other studies using the U-shaped transpancreatic suture technique reported thus far (57.2% to 66.7%). In contrast, the frequency of bile duct and ampullary cancer (28.4% and 29.1%, respectively) was greater than in other reports [101125]. The relatively higher rate of grade B (9.7%) POPFs in our study compared with other series using similar techniques may be explained by their higher frequency in nonpancreatic diseases.
Bleeding from a gastroduodenal artery pseudoaneurysm is one of the primary causes of mortality and is usually associated with a grade C fistula [27]. In our study, 1 case (1.9%, 1/52) of hemorrhaging from a gastroduodenal artery pseudoaneurysm was associated with a grade C fistula in DM group, whereas no gastroduodenal artery pseudoaneurysms occurred in the IM group. Despite the lack of statistical significance, the absence of bleeding from gastroduodenal artery pseudoaneurysms in the IM group shows that the IM technique can reduce the risk of gastroduodenal artery pseudoaneurysms by decreasing the incidence of grade C fistulas.
In summary, our study showed that the inverted mattress PJ method effectively decreased the risk of grade C pancreatic fistulas and subsequent serious complications, such as gastroduodenal artery pseudoaneurysms.
Inverted mattress end-to-side PJ shortened operation time and increased safety with no incidence of grade C POPF or bleeding from gastroduodenal artery pseudoaneurysms.



 XML Download
XML Download