

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nonalcoholic fatty liver disease affects 10%-30% of adults and 13% of children in the general population [1,2]. In living donor liver transplantation (LT), a fatty donor liver is associated with increased morbidity in both recipients and donors. Grafts with greater than 30% steatosis may be nonfunctional, and steatosis in the remaining liver impacts the recovery of donors after hepatectomy [3,4]. Therefore, an accurate and precise quantification of fat content is essential for assessing the eligibility and safety of potential donors [5].
There are several methods to evaluate hepatic fat content. Biopsy was known as the gold standard in quantifying liver steatosis. However, it is invasive and can cause bleeding, infection, and bile leakage in healthy living donors. Another problem is sampling error [6].
Semiquantitative noninvasive methods include CT visual grading [7], liver/spleen attenuation ratio, and liver attenuation index (the difference of attenuation between liver and spleen) in nonenhanced CT [8]. And ultrasonography has been also used, but these are useful only for the detection of moderate and severe degrees of steatosis.
Recently magnetic resonance (MR) chemical shift imaging (CSI), and MR spectroscopy (MRS) are considered to be the most accurate noninvasive methods to measure fat content of the liver [4]. Limitations of MR imaging include variations due to differences between MR imaging systems, scanning parameters, and methods of analysis. In addition, it is relatively expensive and suffers from lower diagnostic performance in estimating hepatic fat content in cases with iron deposition [9,10]. In spite of these limitations, high levels of correlation between fat fraction using CSI or MRS and the results of liver biopsy are well described [11,12,13]. CSI is more advantageous than MRS in that it requires a short image acquisition time, and one scan supplies enough data to quantify the fat content in any part of the liver. This capability of CSI promises to be useful for evaluation of uneven hepatic fat deposition in living liver donors.
It is not rare to find various pattern of hepatic fat deposit including focal fat deposition, diffuse deposition with focal sparing, multifocal deposition, perivascular deposition, and subcapsular deposition of fat [4,14,15,16,17]. This implies the possibility of error in analyzing the amount of fat in the liver remnant if only a small area of the liver is assessed.
This study assessed the pattern of hepatic steatosis using CSI quantification in the evaluation of potential liver donors, and evaluated the difference between liver biopsy and the estimated fat fraction based on CSI in the same region.
METHODS
We analyzed retrospectively 88 consecutive living donor LTs that were performed at a single center between June 2011 and February 2012. Inclusion criteria were biopsy of the surface of segment 5 during donor operation and CSI performed within 32 days of LT (except 3 cases with CSI images 77, 42, and 45 days before LT). Three donors who underwent left hepatectomy with a biopsy of the surface of the left lobe and another 4 donors who did not have CSI images were excluded, leaving 81 donors who had the results of liver biopsy and CSI images. This study was approved by Seoul National University Hospital (No. 1305-622-491) and followed the ethical guidelines.
MRI and three-point Dixon technique
MRI was performed on a 3.0 T MR imaging system (Siemens Medical Solutions, Erlangen, Germany). An axial, triple-echo, Dixon water-fat separation image with T2* correction was acquired using a 3D gradient echo prototype sequence provided by the manufacturer (Siemens Healthcare, Erlangen, Germany). The triple echo data consisted of in-phase (360 degrees)/opposed-phase (540 degrees)/in-phase (1,080 degrees) images and the imaging parameters were: relaxation time, 9.9 m/sec; echo times of triple echoes, TE1/TE2/TE3 2.5/3.7/7.3 m/sec; flip angle, 11 degrees; matrix, 256 × 167; slice thickness, 3.5 mm (56 slices); and field of view, 380 mm × 327 mm. A single, continuous region of interest (ROI) was defined in each of the source images by including a maximum amount of liver parenchyma, avoiding major blood vessels. From the calculated water-only and fat-only images, hepatic fat fraction images were obtained.
Measuring fat fraction on CSI
All images were interpreted on a Picture Archiving and Communication System (Marosis m-view 5.4, Marotech, Seoul, Korea) that allowed the extraction of fat fraction and T2 maps fitted on a pixel-by-pixel basis. The estimated fat fraction was equal to one-tenth of the mean value in the ROI on the image.
The fat fraction was estimated in 13 different areas: (S1, S2, S3, the peripheral and deep regions of S4, S5, S6, S7, S8). The peripheral and deep regions were arbitrary demarcated at a level 2/3 the distance from the caudate lobe to the liver surface. To estimate fat fraction in the peripheral regions and deep regions of the liver, an ROI of approximately 1-2 cm2 was drawn in each region. ROIs in the peripheral region of S4, S5, S6, S7, S8 were long, narrow freehand ROIs drawn along the liver surface. Circular ROIs, avoiding hepatic and portal veins, were used in the deep regions of the same segments (Fig. 1). However, because of their size, S1, S2, and S3 could not be divided into peripheral and deep regions. The fat fraction in each area was the average of three fat fractions measurements taken on 3 different consecutive axial images.
Liver biopsy
Liver wedge biopsy was routinely performed during donor hepatectomy. The biopsy site was the anterior edge (peripheral region) of S5 in our center. Biopsy specimens were approximately 0.5 cm × 0.5 cm × 0.5 cm in size. The degree of macrovesicular and microvesicular steatosis was reported on a percentage scale using hematoxylin and eosin stained sections by a liver transplant pathology specialist. Its quantification relies on the visual estimation of percentile hepatocytes that have the macrovesicular or microvesicular lipid vacuoles.
Range of fat fractions in the liver
Range of fat fractions was defined as the difference between the maximal value and the minimal value among the 13 measured fat fractions in the liver.
Range of fat fraction in the whole liver according to the peripheral fat deposit
Individual range of fat fraction according to the fat fraction in peripheral region of S5 (biopsy site) was analyzed to predict the change of fat accumulation pattern on the amount of peripheral fat deposit.
Statistical analysis
Correlations between the estimated fat fraction using CSI, the histologic degree of macrovesicular fatty change in the biopsy, and the range of fat content in the 13 ROIs were assessed with Pearson correlation, the paired t-test, linear regression, and analysis of variance (ANOVA). After analysis with repeated measures of ANOVA, Bonferroni adjustment was applied to control for type I error. All statistical analyses were performed using commercial software IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). A P-value of ≤0.05 was considered significant.
RESULTS
The mean age of donors was 31.9 (standard deviation [SD], 11.4) years and mean BMI was 23.7 (SD, 2.7) kg/m2. Male gender was predominant (75.3%) and mean macro-vesicular fat change was 3.24% (SD, 4.6) on liver biopsy. Table 1 shows the average estimated fat fraction in all 13 regions using CSI. The estimated fat fraction in the peripheral region of S5, where liver wedge biopsy was performed during donor operation, correlated well with the amount of macrovesicular fatty change in the biopsy samples (r = 0.816, P < 0.001). They showed a linear correlation (Fig. 2) (R2 = 0.667, P < 0.001).
There was a significant difference in fat fractions between the peripheral and deep regions of S4, S6, S7, and S8, with a higher fraction peripherally: S4 (3.8% ± 2.7% vs. 3.1% ± 2.8%, P < 0.001), S6 (3.6% ± 3.7% vs. 3.4% ± 3.6%, P = 0.004), S7 (3.9% ± 2.8% vs. 3.3% ± 3.4%, P < 0.001), and S8 (3.7% ± 3.4% vs. 3.3% ± 3.0%, P = 0.006). The value of the fat fraction in peripheral regions (A) minus the fat fraction in deep regions (B) varied from -4.8 to 5.3. The absolute maximal difference in values was 4.1%, 4.9%, 3.2%, and 5.3% in S4, S6, S7, and S8, respectively (Table 2).
The deep regions of S4-S8 and S1-S3 had statistically different fat fraction values from one another (F [4.003, 58.032] = 8.684, P < 0.001), while there were no differences in the amount of accumulated fat fraction among the peripheral regions of S4, S5, S6, S7, and S8 (F [2.9, 5.3] = 1.3, P = 0.272).
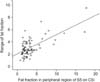
Additionally, the range of the fat fraction in the whole liver increased as the value of the fat fraction in the peripheral region of S5 on CSI increased (Pearson correlation = 0.654, P < 0.001, R2 = 0.428) (Fig. 3).
DISCUSSION
The assessment of hepatic steatosis is important in preoperative evaluation of living liver donors. As the degree of macrovesicular fatty change in the liver is associated both with recipient graft function and donor recovery, accurate and precise quantification of hepatic fat content is essential preoperatively. Because it is well known that distribution of fat is uneven in the liver, it is questionable whether a liver biopsy and imaging studies to quantify fat content in a small area of the liver can reflect the rest of the liver exactly.
With the development of MRI techniques for evaluation of fat content, such as CSI and MRS, we can quantify fatty change in the liver noninvasively. Considering that donor safety is paramount in living donor LT, if a noninvasive imaging technique such as CSI or MRS can measure the precise amount of fat in the whole liver, it would be a useful workup tool for living liver donor candidates. Until now, there have been only a limited number of studies exploring the utility of such techniques in preoperative evaluation of living liver donors [13,18,19].
The results of this study show that there is a linear relationship between the fat fraction measured with CSI in the peripheral region of S5 (biopsy site) and histological fatty change on biopsy. This means that fat fraction of the liver estimated from CSI reflects the regional pathologic fatty change directly, as several papers which demonstrated the value of CSI or MRS for evaluation of hepatic steatosis in the general population have pointed out [4,11,13,20].
MRS and CSI are accurate methods to estimate hepatic fat fraction because they exploit differences in resonance frequencies of fat and water signals. However, MRS has several limitations: First, it cannot estimate the fat fraction in several regions of the liver at one time. Second, the region to be estimated is usually limited to a small area. Third, its signal can be influenced by hepatic iron content. In this context, previous studies have demonstrated that CSI using a modified Dixon method for quantification of fat in the liver may overcome these limitations. It has the advantages of easy manipulation, whole liver coverage, minimal vulnerability to iron content, and the absence of radiation. Based on our study results, we can propose that CSI with triple echo is a useful technique in evaluation of living liver donors, as it can provide quantification of fat fraction for any region of the liver. Considering that MR examination is widely used for preoperative evaluation of the biliary anatomy in living liver donor candidates, adding CSI to an MR cholangiopancreatography examination would not require further expense, and also requires only one breath-hold examination of 19 seconds.
We estimated fat fractions in 13 different regions of the liver using CSI with triple echo technique. This study showed that the distribution of hepatic fat was heterogeneous with objective data. There was a significant difference in fat fractions between the peripheral regions and deep regions of the same segments. While the fat fractions in the peripheral regions of S4-S8 were not different from one another, the amount of hepatic fat in the deep regions showed significant differences with other segments in deep region. Fig. 4 shows the example of differences in fat fraction between the deep regions of S7 and S8.
We showed that that increased fatty change was associated with greater heterogeneity of the fat fraction. This implies that the estimated value of fat fraction in a specific region could be different significantly from the fat fraction in other parts of the liver, according to the degree of overall fat content. On the basis of our results, we believe that a needle or a wedge liver biopsy or an estimated fat fraction using an MRI technique with a small sampling volume (such as MRS) cannot represent the remaining liver completely, especially in patients with severe fatty liver.
For the safety of both donor and recipient, we have to know the exact status of the liver graft as well as the remnant liver before LT. Because the accuracy of liver graft fatty change measurement is important, predicting fatty change of the remaining liver may lead to sampling error if based on information from a biopsy or a small area of regional fat fraction measurement, especially with a severely fatty liver. We suggest that multifocal estimation of hepatic fat is needed in the evaluation of donor candidates, especially with severe steatosis. Although liver biopsy is still useful to exclude liver disease such as steatohepatitis, CSI, which allows multiregional evaluation for steatosis, would compensate for the limitation of pathologic assessment for steatosis using needle or wedge biopsy. Further study is warranted to determine whether CSI can reduce the necessity for liver biopsy in the population at large and focal fat deposit would be related with focal steatohepatitis.
This study has certain limitations. First, only 13 patients with 5% macrovesicular fatty change or over were included in our study because of our selection criteria specific to donors. Second, only potential risk without clinical outcomes with hepatic fat heterogeneity was suggested. Third, CSI imaging does not differentiate macrovesicular fatty change from microvesicular fatty change because it uses only the difference of signal resonance between water and fat.
Despite that, this study yielded important information. First, it showed that the distribution of liver fat is heterogeneous with objective quantitative data from MRI. Second, fatty change in a specific small region might not reflect the concentration in the remaining liver, especially severe steatosis. Third, range of fat deposition in the whole liver increases with the overall amount of hepatic fat content. Fourth, the estimated fat fraction on CSI showed good correlation with pathological fat fraction in the same region.
Therefore, a needle or a wedge liver biopsy or estimated fat fraction using MRI technique with small sampling volume cannot represent the remaining liver, especially in patients with severe hepatic steatosis. Multifocal fat measurements for the whole liver are needed to determine the exact fatty change of the liver.





 XML Download
XML Download