

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lymphangiomas are usually located in the head and neck area as well as the abdominal wall, but rarely in the mesentery [1]. Although mesenteric lymphangiomas can occur at any age, they are present at birth in 65% of all patients and nearly 60% of all patients are diagnosed before the age of 5 years [23]. The incidence of mesenteric lymphangioma is about 1 in 20,000 pediatric hospital admissions in the United States [4]. Most mesenteric lymphangiomas are initially asymptomatic, but some patients complain of vague subjective symptoms, such as pain, nausea, vomiting, or alterations in bowel habits depending on the size and location of the lymphangiomas [34]. Lymphangiomas should be treated through complete resection because they can cause bleeding or infection as well as invasion of vital structures [3]. After excision of a mass that involves the whole mesentery, internal herniation is likely to occur through the skeletonized vessels. We used a biologic collagen implant (Permacol, Covidien, Norwak, USA) to repair the mesenteric defect after excision of a huge mesenteric lymphangioma and followed up for 4 years.
CASE REPORT
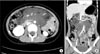
An 11-year-old girl was referred to Seoul National University Children's Hospital with pain in the right lower quadrant of the abdomen that began 2 months prior to admission. She did not have a specific past medical history, and did not report either fever or any other relevant gastrointestinal symptoms, such as anorexia or vomiting. On physical examination, the patient had mild tenderness in the right lower quadrant of the abdomen. A fixed mass was palpable around the periumbilical region. No other specific findings were noted in the laboratory tests, including complete blood counts, and C-reactive protein. CT revealed an infiltrative cystic mass in the mesentery measuring 10.5 cm × 8.7 cm × 7.5 cm, and that the small bowel was displaced laterally and inferiorly due to the mass (Fig. 1).
The radiological diagnoses included mesenteric lymphangioma, lipoblastoma, and neurogenic tumor. Exploratory laparotomy demonstrated a broad-based multiple cystic lymphangioma within the mesentery ranging from the Treitz ligament to the transverse colon (Fig. 2A). However, it did not involve the surrounding viscera. The lymphangioma was excised nearly completely saving mesenteric vessels by skeletonization. As a result, a very large-sized mesenteric defect from that of the jejunum to the transverse colon with centrally skeletonized vessels developed. Initially, we tried to close the defect without implant, but failed, because the intestine and vessels came to be angulated and lead to obstruction. The mesenteric defect was repaired with a Permacol (Fig. 2B). Histopathologic findings were consistent with mesenteric lymphangioma. On postoperative day 7, the chyle leak was developed through the drainage tube and was resolved by conservative management. The patient was discharged from the hospital on postoperative day 17 without other problems from the biomaterial implant.
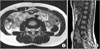
She was regularly checked with ultrasonography, CT, and MRI at our outpatient clinics. After 3 months, abdominal CT revealed a residual lymphangioma around the head of the pancreas and the portal vein. The implant did not cause any problems. At a recent follow-up, 4 years after operation, abdominal MRI did not showed any changes from 3 months postoperative status (Fig. 3). During the follow-up period, she has been doing well without complaint of any symptoms.
DISCUSSION
A standard treatment of huge mesenteric lymphangioma has not yet been established due to its very low incidence. However, surgical excision is necessary because it invades adjacent organs and can cause infection or bleeding [3]. In this case, we performed surgical resection of the huge mesenteric lymphangioma because of abdominal pain and invasion to the adjacent organs.
As in our case, excision of a huge lymphangioma may create mesenteric defects of various sizes, which can cause internal herniations that result in intestinal volvulus and obstruction. Some authors suggested that patients with segmental mesenteric defects require intestinal fixation and resection of the affected intestine [5]. De la Cruz-Munoz et al. [6] reported that the incidence of internal hernia decrease through the closure of mesenteric defects. However, controversy exists regarding closure of the mesenteric defect in specific circumstances. Cabot et al. [7] reported that mesenteric defects are not associated with significant rates of relevant internal hernia in specific operations, such as laparoscopic right hemicolectotomy and laparoscopic Roux-en-Y gastric bypass.
The use of an implant for the empty space is another solution. There are two available materials for mesenteric repair including synthetic meshes and biologic collagen implants. Synthetic meshes, such as polyprophylene implants, are commonly used, but they have limited tissue-incorporation abilities as well as an increased risk of complications, such as adhesion, erosion, or fistula formation [89]. To overcome the shortcomings, attention has recently been focused on biological implants derived from allogenic or xenogenic sources [10]. Permacol is a sheet of porcine dermal collagen. Cross-links between collagen fibers give it its durability by preventing collagenase destruction. It gradually remodels human tissue while preserving its structural integrity. Moreover, porcine dermal implants induce minimal inflammation and adhesion even when they come into direct contact with viscera [89]. Although porcine dermal implants have a disadvantage of forming intra-abdominal abscess or sepsis in contaminated circumstances, they have widely been used for abdominal wall repair, chest wall repair, and reconstruction surgery and have proved to be stable [10]. In this case, Permacol also did not showed any complications for 4 years.
In summary, to avoid internal herniation through a large mesenteric defect, after excision of huge mesenteric lymphangiomas, closure with implant would be a good choice, and Permacol would be a possible implant for closing the defect. To the best of our knowledge, this is the first case on the use of Permacol for a huge mesenteric defect in children.

 XML Download
XML Download