

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Secondary hyperparathyroidism (SHPT) indicates excessive secretion of parathyroid hormone (PTH) by the parathyroid glands in response to hypocalcemia and associated hypertrophy of the glands [1]. SHPT frequently develops in patients with chronic renal failure. During renal failure, the serum calcium level is decreased because the failing kidneys are unable to convert enough vitamin D to its active form. In addition, the failing kidneys could not adequately excrete phosphate, phosphate retention occurs and causes hypocalcaemia. In response to hypocalcaemia, the parathyroid glands are stimulated with increased secretions of PTH. SHPT leads to the restoration of serum calcium level via the mobilization of calcium from the bones to the blood stream, and partial correction of hyperphosphataemia. Therefore, SHPT is regarded as a biological adaptation response to restore normal blood calcium levels at the expense of increased serum PTH [2].
Based on the pathogenesis of SHPT, great effects have been taken to develop effective therapeutic agents for SHPT such as calcimimetics, phosphate binders, and less calcemic vitamin D analogues. However, parathyroidectomy is needed for some patients with long-standing SHPT [3]. Currently, subtotal parathyroidectomy and total parathyroidectomy are considered to be the standard surgery procedures for SHPT treatment [4].
For parathyroidectomy, surgical stimulus during the dissection of the gland is mostly gentle and regional anesthesia is enough [5]. However, for some patients with SHPT, relatively deep anesthesia is required, perhaps due to the combination of surgery and frequent tracheal stimulation associated with the movements of the endotracheal tube during the surgery operations. Serum glucose and noradrenaline (NE) levels are good indicators for stress response to surgery. It remains unclear whether anesthesia with superficial cervical plexus block is better than deep cervical plexus block to reduce postoperative pain and relieve stress response in SHPT patients who undergo subtotal parathyroidectomy. Therefore, this study aimed to compare analgesic efficacy in SHPT patients who undergo subtotal parathyroidectomy after anesthesia with superficial versus deep cervical plexus block.
METHODS
Subjects
This study was approved by the Ethics Committee of Shenzhen People's Hospital, and informed consent was obtained from each subject. Sixty chronic renal failure patients with SPHT scheduled for subtotal parathyroidectomy surgery under general anesthesia between April 2011 and February 2013 were enrolled. American Society of Anesthesiologists physical status of the patients was III-IV, serum glucose level was normal, age ranged from 38 to 64 years old, weight ranged from 55 to 69 kg, height ranged from 155 to 172 cm. Those patients who had mental diseases or had taken monoamine oxidase inhibitors were excluded from this study.
By a random number sequence, 60 patients were randomized to receive only general anesthesia (group GA), general anesthesia plus bilateral superficial and deep cervical plexus block (group BD), or general anesthesia plus bilateral superficial cervical plexus block (group BS), and each group included 20 patients.
Surgical procedures
For general anesthesia, all patients were administrated with intravenously propofol, fentanyl, cisatracurim, oral cuffed endotracheal tube, anesthesia was maintained with oxygen 50%, nitrous oxide 50%, sevoflorane, mechanical ventilation with maintenance of endtidal carbondioxide 35-40 mmHg. After the induction of general anesthesia, cervical plexus blocks were performed bilaterally by an anesthesiologist unaware of the solutions injected. For deep block, a 23-gauge, short-beveled needle was inserted behind the lateral border of the sternocleidomastoid muscle, 3-cm distal to the mastoid process, then 10 mL of 0.5% ropivacaine was administered bilaterally (5 mL each side). The superficial block was performed by using the same needle inserted at the midpoint of the lateral border of the sternocleidomastoid muscle, then 10 mL of 0.5% ropivacaine was administered bilaterally (5 mL each side) to block the main branches of the plexus. The specific treatment given was unknown to the patient, anesthesiologist, surgeon, or nurse in charge of pain assessment. The postoperative pain was assessed using visual analogue scale (VAS), with score 0 corresponding to no pain and score 10 to the maximum pain. Then patient-controlled analgesia (PCA) pump was programmed to deliver tramadol of 400 mg in 92 mL of 0.9% saline, lockout interval 15 minutes, no background infusion, 5 mL per pump.
RESULTS
General parameters in three groups
As shown in Table 1, we found no significant differences in the gender, age, weight, operation time, bleeding volume, and infusion among the three groups (P > 0.05).
Serum glucose and NE levels in three groups
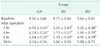
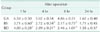
At baseline, there were no significant differences in serum glucose and NE levels among the three groups (P > 0.05) (Tables 2, 3). At 1 hour, 4 hours, and 8 hours after operation, serum glucose and NE levels were significantly higher than baseline (P < 0.05), but serum glucose and NE levels at 24 hours after operation showed no significant differences from those at baseline (P > 0.05).
Hemodynamic changes in three groups
We compared hemodynamic parameters in three groups such as systolic blood pressure, diastolic blood pressure, mean arterial blood pressure, and heart rate. As shown in Table 4, these parameters showed no significant differences at baseline among the three groups (P > 0.05). In GA group, hemodynamic parameters at 1 hour, 4 hours, and 8 hours after operation were significantly higher than those at baseline (P < 0.05). In BD and BS groups, hemodynamic parameters at 1 hour, 4 hours, and 8 hours after operation were slightly higher than those at baseline, but showed no significant differences (P > 0.05). In addition, hemodynamic parameters at 1 hour, 4 hours, and 8 hours after operation were significantly different between GA group and BD and BS groups (P < 0.05). However, at 24 hours after operations, hemodynamic parameters in all groups were not significantly different from those at baseline (P > 0.05).
VAS score in three groups
We analyzed VAS score after the operation in three groups. The results showed that VAS score at 1 hour, 4 hours, and 8 hours after operation was significantly lower in BS and BD group than in GA group (P < 0.05), but there was no significant difference in VAS score in three groups at 24 hours after operation (P > 0.05) (Table 5).
Dosage of tramadol in three groups
For PCA, the duration was the same in all three groups. The frequency was 15.1 ± 1.36 in GA group, 5.5 ± 1.76 in BS group and 4.7 ± 1.13 in BD group. The total dose of tramadol used was 300.0 ± 27.13 mg in GA group, 109.0 ± 35.2 mg in BS group and 93.0 ± 24.52 mg in BD group. The frequency and dosage of tramadol were significantly higher in GA group than in BS and BD group (P < 0.05).
Complications in three groups
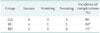
Within 24 hours after operation, complications developed in three groups (Table 6). We found that each type of complication belonged to different patients, and the number of patients with complications was significantly higher in GA group than in BS and BD group (P < 0.05).
DISCUSSION
Surgical procedure is known to stimulate a series of hormonal, metabolic and inflammatory changes that together form stress response [6]. Under stress response, sympathetic-adrenal medullary system is stimulated and serum catecholamine level increases. On the other hand, hypothalamic-pituitary-adrenal axis is stimulated, leading to glucocorticoid secretion and the increase in serum glucose level [7]. Consistent with the theories, in this study we found that serum glucose and NE levels were significantly higher at 1 hour, 4 hours, and 8 hours after operation, compared to baseline, but serum glucose and NE levels returned to baseline levels at 24 hours after operation, indicating that stress response is finished by then.
Analgesia efficacy after general anesthesia alone is not ideal and most patients require postoperative analgesia [8]. Inadequate relief of postoperative pain will lead to increased levels of stress hormones and increased incidence of perioperative complications. Long-acting local anesthetic anesthesia combined with cervical plexus block could help reduce the pain after surgery and the stress response, and restore the hemodynamics in patients after surgery [9]. In this study, we used ropivacaine which is a long-acting local anesthetic agent. Compared to bupivacaine, ropivacaine has low cardiac toxicity and great advantages in cervical plexus blockade [10]. Kim et al. [11] reported that the use of ropivacaine for combined deep and superficial cervical plexus blockade could reduce joint vagal reflex, enhance cardiovascular function, and was suitable for patients with high risk of cardiovascular disease. Several studies have shown the sucessful application of ropivacaine for superficial or deep cervical plexus blockade to achieve analgesia after parathyroidectomy [121314]. In particular, Cai et al. [13] found that bilateral superficial cervical plexus block with ropivacaine before surgery significantly reduced the incidence of postoperative nausea and vomiting and postoperative pain. In agreement with this, in this study we observed that bilateral superficial and deep cervical plexus block or bilateral superficial cervical plexus block led to reduced incidences of complications such as nausea and vomiting and reduced VAS score.
Notably, Suh et al. [15] compared the analgesic efficacy of bilateral superficial cervical plexus block and combined superficial and deep cervical plexus block for incision pain, headache and posterior neck pain after thyroidectomy, and their results suggested that superficial cervical plexus block is more effective than combined superficial and deep cervical plexus block to reduce the pain during and immediately after thyroidectomy. In this study, we found that there was no significant difference in postoperative pain and the number of patients with complications between BS group and BD group.
In summary, the results of the present study show that under general anesthesia superficial cervical plexus block or combined superficial and deep cervical plexus block can effectively reduce postoperative pain and stress response in chronic renal failure patients with SHPT who undergo subtotal parathyroidectomy, and significantly reduce the incidence of complications such as nausea and vomiting. In comparsion, superficial cervical plexus block and combined superficial and deep cervical plexus block show no significant difference in analgesic efficacy, but bilateral superficial cervical plexus block is safer than combined bilateral superficial and deep cervical plexus block and may be more appropriate for clinical application.



 XML Download
XML Download