

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Paraduodenal hernia (PDH) is by far the most common form of congenital internal hernia, accounting for up to 53% of all reported cases [1]. Left PDHs are three times more common than their right-sided counterparts. The lifetime risk of bowel incarceration associated with PDH is around 50% [2]. Bowel incarceration can result in increased morbidity and mortality. Therefore, PDHs should be treated if found incidentally.
Chylous ascites is an accumulation of lymphatic fluid in the peritoneal cavity. It develops when the lymphatic system is disrupted due to traumatic injury or obstruction [3]. We present a unique case of PDH with development of chylous ascites that presented as acute abdomen.
CASE REPORT
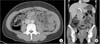
A 40-year-old, previously healthy woman presented to the Emergency Department with severe, colicky abdominal pain. The pain started 2 hours before her visit, with a numeric rating scale score of 10 out of 10. It intermittently recurred and radiated to the back. It was not related to food intake and not associated with fever, chilling, nausea, vomiting, and diarrhea. It was her first time to experience such a pain. After intravenous administration of analgesics, the pain subsided. On physical examination, her bowel sound was normoactive, and her abdomen was soft and flat. Tenderness and rebound tenderness were observed at the left upper and lower quadrants of the abdomen. In the initial laboratory test, no abnormal results and evidence of inflammation were found, with a white blood cell count of 4,000 × 103/µL and neutrophil level of 52%. An abdominal film did not reveal any evidence of bowel obstruction. Abdominal CT confirmed a cluster of dilated proximal small bowel loops with ischemic change, without ascites (Fig. 1).
The patient underwent an emergency surgery to relieve bowel ischemia in 8 hours. As soon as the peritoneum was exposed, 1.5 L of chylous fluid was found even though there was not any pre-existing evidence of ascites. A hernial sac was found along the posterior side of the mesentery of the inferior mesenteric artery (Fig. 2). We resected the hernial sac and pulled out the herniated small bowel. The herniated small bowel mesentery had a whitish discoloration caused by lymphatic leakage. On whole-bowel exploration, the color of the small bowel was normal, and there was no sign of ischemia or strangulation. Massive irrigation was performed, and a Jackson-Pratt drain was inserted. We tested for chylous ascites and measured the triglyceride level, which was 766 mg/dL. On the sixth day after the surgery, she was discharged without any complication.
DISCUSSION
In 1923, Andrews (quoted from [4]) proposed that PDH forms as a result of a congenital anomaly in the development of the peritoneum that arises during midgut rotation [4]. As a consequence, the small bowel becomes invaginated into an avascular, and therefore unsupported, segment of the left mesocolon. The resulting small bowel thus becomes trapped between the posterior abdominal wall, with the mesocolon and inferior mesenteric vein forming the anterior wall of the hernial sac.
A left PDH contains most of the small bowel, with the afferent limb being the fourth part of the duodenum and the efferent limb being the terminal ileum. The small bowel invaginates into the fossa of Landwert, which lies to the left of the fourth portion of the duodenum [5]. Treatment of PDH follows the basic principles of hernia surgery as follows: reduction of the contents, resection of the hernial sac, restoration of normal bowel anatomy, and repair of the hernial defect. Timely surgical intervention is important because of the 50% lifetime risk of bowel incarceration [6].
In a review article of adult patients, chylous ascites were reported to be more commonly caused by malignancy, liver cirrhosis, tuberculosis, abdominal surgery, and trauma [3]. Chyle is distinguished by its odorless milky appearance, which is similar to peripheral lymphatic fluid. The triglyceride concentration of chyle is typically 2-8 times higher than that of plasma (>200 mg/dL). Fat globules present in chyle stain positive with Sudan red stain. In normal physiology, the gut lymphatics carry converted long-chain triglycerides from the intestine to the vascular system via the thoracic collection duct at a rate of 50-200 mL/kg/hr [7]. Hence, in cases of acute lymphatic obstruction, rapid accumulation of chyle can occur. In 1976, Kinmonth [8] first described a case of lymphatic flow disruption that caused chylous ascites. Koh et al. [9] postulated that intestinal malrotation causes lymphatic flow obstruction, which leads to the exudation of chyle and the eventual accumulation of chylous fluid. They reported that after the mesenteric torsion was treated soley, the chylous ascites was spontaneously resolved. In our case, the chylous ascites would have developed through acute lymphatic obstruction due to pressure trauma in the restricted hernial sac and it was treated spontaneously via surgical correction of the PDH.
In conclusion, we think that in our case, the left PDH resulted in small bowel obstruction and ischemia, which caused the severe abdominal pain. We found that chylous ascites was developed due to lymphatic flow obstruction on the CT, which led to the exudation of chyle from the herniated bowel. Drainage of the chylous ascites decreased the bowel pressure, and the small bowel recovered from the ischemia.

 XML Download
XML Download