

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laparoscopic cholecystectomy (LC) has become a mainstream modality in patients with benign gallbladder disease [1]. With the technical advancement in LC, cosmetic outcomes have improved and postoperative scars have been minimized. Single incision laparoscopic cholecystectomy (SILC) was first report by Navarra et al. [2] in 1997. Since then, it has been widely used based on its advantages [3]. That is, as compared with conventional LC (CLC), SILC is a more advantageous modality in that it causes less postoperative scars and pain. It is disadvantageous, however, in that it prolongs operation time, causes postoperative complications and incurs a higher cost [34567]. This limits the applicability of SILC as a standard treatment modality.
Several studies have introduced various methods of SILC [28910], but a standard method of SILC has not been established yet. We have previously reported that we performed a 3-channel SILC. The exposure of Calot's triangle and performing "critical view of safety" posed a challenging problem [1112]. We have therefore introduced another instrument, a snake retractor for retraction of liver [13]. Thus, we have performed a total of 722 cases of SILC.
In this study, we compared the surgical outcomes of 3-channel and 4-channel SILC performed in our hospital. And we evaluated the risk factors for prolonged operative time in SILC.
METHODS
Study patients and setting
Between April, 2010 and August, 2014, we performed a total of 722 cases of SILC at Konyang University Hospital. We collected the data through a retrospective analysis of medical records. Between April, 2010 and September, 2012, we performed 323 cases of 3-channel SILC. Between October, 2012 and August, 2014, we performed 399 cases of 4-channel SILC after the introduction of a snake retractor for liver retraction. We named the 3- and 4-channel SILCs as Konyang standard method (KSM) and modified KSM (mKSM), respectively. All operations were performed by two hepatobiliary surgeons.
In the earlier period, we excluded such cases as patients aged 70 years or order, patients who concurrently had cardiopulmonary disorder, patients with acute inflammation, and patients who were suspected of having malignancy [11]. After performing 50 cases of SILC, as our experience had accumulated, we applied SILC to all benign gallbladder diseases. Thus, we modified our exclusion criteria to only the patients who were suspected of having malignant gallbladder diseases.
Surgical technique and instruments
The surgical glove and Alexis wound protector (Applied Medical, Rancho Santa Margarita, CA, USA) were used to create a hand-made umbilical port. We used a flexible laparoscope (Olympus Co., Tokyo, Japan), long articulated laparoscopic instruments (Covidien, Mansfield, MA, USA), and a snake retractor (DiamondFlex Triangular Retractors, CareFusion, Waukegan, IL, USA). Thus, we made a 2.5-cm transumbilical incision and inserted a laparoscope in the handmade port. After making pneumoperitoneum, we arranged the flexible telescope, snake retractor and endoscopic instruments as previously described. The patients were placed in a reverse Trendelenburg position at an angle of 15°-30° with the right side up. Gallbladder was retracted laterally with a grasper using the right hand, through the 1st finger of the handmade port, and the anterior peritoneum surrounding the cystic duct was dissected by a dissector using the left hand through the 5th finger of the handmade port. This was followed by posterior dissection using the right hand grasper. After isolating the cystic duct and artery, we clipped them using the 5-mm HemOLok (Weck Closure Systems, a division of Teleflex Inc., Wayne, PA, USA) and then divided them. Following the dissection of gallbladder from the gallbladder bed, we performed an irrigation using a suction-hook bovie (Endopath Probe Plus II Pistol Grip Handle, Ethicon EndoSurgery Inc., Cincinnati, OH, USA). Then, the gallbladder was removed through the Alexis wound retractor positioned at the umbilical incision without an endobag. All the procedures of 3- and 4-channel SILC were done as previously described. [1113].
Outcomes measures
In the current study, we performed a retrospective analysis of baseline and demographic characteristics of the patients. These characteristics include age, sex, body mass index (BMI), a past history of abdominal operation, the American Society of Anesthesiologists scores, preoperative percutaneous transhepatic gallbladder drainage (PTGBD) insertion, surgeons' technical expertise, operation time, estimated blood loss, drainage insertion, length of hospital stay, histopathologic findings, conversion to open or conventional laparoscopic surgery and postoperative complications. The operation time was defined as the interval from initial skin incision to final skin closure and the time preparing the glove port was not included. All the complications were recorded according to the Clavien-Dindo classification [14].
Statistical analysis
Statistical analysis was done using the PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA), for which we performed chi-square test, Student t-test, and univariate and multivariate logistic regression analyses. The operation time was expressed as mean ± standard deviation, which served as a cutoff value. In addition, operation time was determined to be long when its mean value was greater than the cutoff value. To identify potential predictive factors of prolonged operation time, we performed multivariate analysis using a logistic regression model. A P-value of less than 0.05 was considered statistically significant.
RESULTS
Baseline and clinical characteristics
Our clinical series of patients comprise 332 men (46.0%) and 390 women (54.0%), whose mean age was 52.4 ± 14.8 years. The number of patients who had a past history of abdominal surgery and upper abdominal surgery was 177 (24.5%) and 18 (2.5%), respectively. There was no significant difference in the number of the patients with a past history of upper abdominal surgery between the two groups (9 [2.5%] vs. 9 [2.3%], P = 0.859). Overall mean BMI was 24.7 ± 3.6 kg/m2. There was a significant difference in the number of the patients who had a past history of preoperatively taking PTGBD between the two groups (31 [9.6%] vs. 66 [16.5%], P = 0.007). Clinical characteristics of the patients are represented in Table 1.
Surgical outcomes
Operative factors and surgical outcomes are shown in Table 2. Mean operation time was significantly shorter in the KSM group as compared with the mKSM group (51.7 ± 20.1 minutes vs. 55.8 ± 19.7 minutes, P = 0.006). The estimated blood loss was significantly greater in the KSM group as compared with the mKSM group (24.6 ± 54.4 mL vs. 16.9 ± 27.0 mL, P = 0.013). The length of hospital stay was 2.9 ± 3.0 days and 2.6 ± 1.6 days in the corresponding order. But this difference reached no statistical significance (P = 0.098). The proportion of patients undergoing drainage insertion was significantly lower in the KSM group as compared with the mKSM group (3 [0.9%] vs. 15 [3.8%] cases, P = 0.016). There was no significant difference in the frequency of conversion to conventional laparoscopic or open cholecystectomy between the two groups (6 [1.9%] vs. 10 [2.5%], P = 0.556).
Postoperative histopathologic findings
With regards to postoperative histopathologic findings, acute cholecystitis or empyema were more prevalent in the mKSM group as compared with the KSM group (56 [14.0%] vs. 28 [8.7%], P = 0.025) (Table 2). Postoperatively, there were three cases of incidental gallbladder cancer in the mKSM group (data not shown).
Postoperative complications
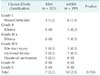
There was no significant difference in the incidence of postoperative complications between the two groups (7 [2.2%] vs. 10 [2.5%], P = 0.765) (Table 2). As shown in Table 3, there were 17 patients (2.4%) who developed postoperative complications. They comprise 7 patients (2.2%) of the KSM group and 10 patients of mKSM group (2.5%). But this difference reached no statistical significance (P = 0.765). In the KSM group, there were 1 case of bile duct injury (grade IIIb), 1 case of duodenal perforation (grade IIIb), 4 cases of wound infections (grade I) and 1 case of incisional hernia (grade IIIb). The patient with bile duct injury was detected at postoperative day 2, for whom we performed hepaticojejunostomy. The patient with duodenal perforation showed peritoneal irritation sign at postoperative day 2, for which we performed laparoscopic primary repair of the perforation site. In the mKSM group, there were one case of bile duct injury (grade IIIb), 6 cases of wound infection (grade I), 1 case of incisional hernia (grade IIIb), and 2 cases of biloma (grades II and III). The bile duct injury was found intraoperatively, so we introduced one additional 5-mm trocar at epigastric area and primary repair was done. There were no deaths in our series.
Risk factors of prolonged operation time
To identify risk factors of prolonged operation time in the patients undergoing SILC, we analyzed the relevant factors. On univariate analysis, BMI, a past history of PTGBD, surgeons' technical expertise, drainage insertion, histopathologic outcomes and operative methods had a significant correlation with prolonged operation time. On multivariate logistic regression, drainage insertion (P = 0.027; odds ratio [OR], 10.245), acute inflammation (P < 0.001; OR, 2.788), surgeons' technical expertise (P = 0.003; OR, 2.418), BMI ≥ 30 kg/m2 (P = 0.041; OR, 1.859), and 4-channel SILC (P = 0.007; OR, 1.557) had a significant correlation with prolonged operation time (Table 4).
DISCUSSION
It is generally known that SILC is a good surgical modality because it has shown better cosmetic outcomes with less postoperative pain as compared with CLC [45815]. A 4-channel SILC might be advantageous in acquiring better operative fields for the exposure of Calot's triangle and liver retraction as compared with a 3-channel one. In the current study, we performed a total of 722 cases of SILC and compared the surgical outcomes between the 3- and 4-channel SILC. Most of the studies in this series have been conducted in a small number of series [161718]. To our knowledge, however, we compared postoperative outcomes between the two modalities in the largest number of patients. Our results might therefore be of great significance.
In the current study, the mean operation time was 53.9 ± 19.9 minutes (51.7 ± 20.1 minutes in the KSM and 55.8 ± 19.7 minutes in the mKSM). Arezzo et al. [15] performed a meta-analysis of published studies, thus reporting that the mean operation time was 58.1 minutes in patients undergoing SILC. Hall et al. [17] also performed a meta-analysis and then reported that the median operating time was 80.75 minutes. Consistent with these reports, our results showed that the operation time was relatively shorter in the patients undergoing SILC using 3- or 4-channel method. But the operation time was slightly longer in the patients undergoing 4-channel SILC as compared with those undergoing a 3-channel one. Presumably, this might be due to the following reasons. First, the incidence of acute inflammation was significantly higher in the mKSM group as compared with the KSM group (14.0 vs. 8.7%, P = 0.025). Second, the frequency of drainage insertion was significantly higher in the mKSM group as compared with the KSM group (3.8 vs. 0.9%, P = 0.016). Third, between two hepatobiliary surgeons, the beginner surgeon performed mainly 4-channel SILC than 3-channel SILC (1 case vs. 68 cases). Fourth, a certain period of time was required for preparing a hand-made glove port and inserting a snake retractor for liver retraction.
Sato et al. [19] reported that higher BMI, acute cholecystitis, and resident as an operator were risk factors of prolonged operation time in patients undergoing SILC. Sasaki et al. [20] also reported that the mean operation time was significantly longer in patients undergoing SILC with acute inflammation of gallbladder than those without it (97.5 minutes vs. 85.0 minutes, P = 0.03). According to Khambaty et al. [3], BMI of > 33 kg/m2 had a significant correlation with a higher frequency of conversion to open or conventional LC and longer operation time. Consistent with these reports, our results showed that BMI ≥ 30 kg/m2 (P = 0.041; OR, 1.859), surgeons' technical expertise (P = 0.003; OR, 2.418), drainage insertion (P = 0.027; OR, 10.245), acute inflammation (P < 0.001; OR, 2.788) and 4-channel SILC (P = 0.007; OR, 1.557) had a significant correlation with the prolonged operation time. We cautiously assumed that patients with higher BMI might require more time to make umbilical incisions, placing hand-made ports, and completing wound closures than normal BMI patients.
Sato et al. [19] also reported that the prolonged operation time was associated with a greater amount of blood loss and longer hospital stay in patients undergoing SILC. This leads to the speculation that both factors might be involved in shortening the operation time and improving postoperative outcomes in patients undergoing SILC. In the current study, however, blood loss was significantly smaller in the mKSM group as compared with the KSM group (24.6 ± 54.4 mL vs. 16.9 ± 27.0 mL, P = 0.013). Thus, we could presume that 4-channel SILC would generate a better operative field for which it makes finer manipulation and bleeding control possible compared to the 3-channel SILC.
In the current study, the overall incidence of postoperative complications was 2.4% (2.2% in the KSM group and 2.5% in the mKSM group). Arezzo et al. [15] reported that it was 12.8%. In addition, Hall et al. [17] performed a meta-analysis of published studies in this series, thus showing that the median incidence of postoperative complications was 7.37%. The incidence of bile duct injury was estimated at approximately 0.4% to 0.5% in patients undergoing CLC [212223]. Our results showed that it occurred at an incidence of 0.3% in each group. One of the late complications of SILC, incisional hernia, was also seen in both groups; it occurred at an incidence of 0.3% in each group. According to Helgstrand et al. [24], trocar hernia occurred at an incidence of 1.6% in patients undergoing LC. Agaba et al. [25] reported that the incidence of port-site hernia rate was 2.9% in patients undergoing SILC. As compared with these reports, our results showed that the incidence of postoperative complications, including bile duct injury and incisional hernia in particular, was lower. It can, therefore be inferred that SILC is a safe, feasible modality in patients with benign gallbladder diseases. Moreover, it would also be mandatory to perform careful and meticulous repair of abdominal closure, which is essential for lowering the risk of postincisional hernia due to the increase in the size of fascia defects in patients undergoing SILC.
The conversion to conventional laparoscopic or open cholecystectomy was seen in 6 cases (1.9%) in the KSM group and 10 cases (2.5%) in the mKSM group. But this difference reached no statistical significance. There was one case of conversion to open cholecystectomy in the mKSM group; it occurred as a result of severe adhesion due to inflammation. Hall et al. [17] reported that a median of 8.55% (range, 1.3%-66.7%) of patients undergoing SILC required more than one additional port. Hirano et al. [26] also reported that there was conversion to CLC in 5.6% (14 of 252) of reported cases. The additional port was introduced, because of insufficient views, dense adhesion, needs for choledochoscope, bleeding, insufficient length to reach the gallbladder-duodenal fistula from the umbilicus [1726]. This is consistent with our results. That is, the reasons for conversion to open cholecystectomy or CLC include 3 cases (0.9%) of bleeding, 2 cases (0.6%) of adhesion due to severe inflammation, 1 case (0.3%) of bile duct injury in the KSM group and 4 cases (1.0%) of bleeding, 5 cases (1.3%) of severe adhesion and 1 case (0.3%) bile duct injury in the mKSM group. These results indicate not only that bleeding and adhesion are major risk factors for conversion but also that a 4-channel SILC is advantageous in acquiring better operative fields and overcoming these factors.
As described earlier, we excluded the patients who were suspected of having gallbladder cancers. We found, however, that there were three patients who were postoperatively diagnosed with incidental gallbladder cancer (1 case of T1a and 2 cases of T2 adenocarcinoma, data not shown). Patients with gallbladder cancer are not recommended to undergo SILC; this is because such patients are at increased risks of cancer seeding due to intraoperative gallbladder perforation. However, the exact correlation of the incidence of gallbladder perforation and risk of gallbladder cancer in patients undergoing SILC has not yet been evaluated. Further studies are needed.
Our results showed that there was variability in the operation time depending on surgeons' technical expertise. In the current study, expert surgeons performed 653 cases of SILC during a mean operation time of 53.1 ± 19.5 minutes but beginners did 69 cases during a mean operation time of 62.0 ± 22.7 minutes. Sato et al. [19] reported that there was no learning curve of SILC. According to Tay et al. [27], however, 19 cases were needed to overcome the learning curve of SILC. Qiu et al. [28] also reported that there was a significant decrease in the operation time when surgeons performed 40 cases of SILC. In the current study, there was no significant difference in the operation time between the first 20 cases and the last 20 cases (59.6 ± 18.5 minutes vs. 54.8 ± 14.7 minutes, P = 0.221). Despite of the lack of prior experiences, these results would assume that surgeons would simply adapt to SILC techniques immediately if they are familiar with CLC, and there would be no significant differences in postoperative outcomes between SILC and CLC.
In conclusion, our results showed that drainage insertion, histopathologic findings (acute cholecystitis or empyema), surgeons' technical expertise, BMI ≥ 30 kg/m2 and a 4-channel SILC were potential risk factors of the prolonged operation time. Thus, among patients with these risk factors, CLC could be considered as well although SILC might be a safer and more feasible modality for benign gallbladder disease.



 XML Download
XML Download