

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It has been demonstrated that routine identification of the recurrent laryngeal nerve (RLN) during thyroid surgery is well accepted by surgeons as a way to preserve the nerve's function. However, the best method to preserve the function of the external branch of the superior laryngeal nerve (EBSLN) still remains controversial [1]. The EBSLNs are important for voice quality. Injury to this nerve during thyroid surgery can manifest as ipsilateral paralysis of the cricothyroid muscle [23]. Clinical symptoms may include: hoarseness, breathy voice, an increase in the rate of throat clearing, vocal fatigue, or diminished vocal frequency range, especially with regards to raising pitch [2]. The amount of EBSLNs identified intraoperatively varies from 10% to 80% [45], while the rate of EBSLN injury reported in the literature is between 5% and 28%, depending on different evaluation methods [3678]. Advances in intraoperative neuromonitoring techniques would allow for RLN and EBSLN identification during thyroid surgery.
Recently, various approaches in endoscopic/robotic thyroid surgery have been practiced worldwide. Previous studies reported advantages in endoscopic/robotic thyroid surgery compared to open thyroid surgery, such as better cosmesis, a quicker return to normal activity, less postoperative discomfort in the neck, and less swallowing disturbances, all leading to a better quality of life [91011]. However, there is little information on neuromonitoring of the EBSLNs during robotic thyroid surgery to preserve voice quality. The present study is a preliminary report describing the technique of neuromonitoring the EBSLNs during bilateral axillo-breast approach (BABA) robotic thyroid surgery. The study was undertaken to evaluate the feasibility of this method and to evaluate the vocal outcome before and after surgery.
METHODS
Ten patients who had undergone BABA robotic thyroid surgery in the Department of Surgery at Seoul National University Hospital (Seoul, Korea) agreed to participate in the present study. They all provided written informed consent during the period of May 2010 to December 2010. Patients with a past medical history of voice disorders, neck irradiation, or neck surgery were excluded from the study. This prospective study was approved by the Institutional Review Board of Seoul National University Hospital (Seoul, Korea). Patient demographics included age, sex, fine-needle aspiration cytology, extent of operation, final pathology, operation time, size of tumor, thyroid volume, and presence of thyroiditis.
Surgical techniques and EBSLN monitoring
The operative technique for BABA has been described in detail elsewhere [12]. All patients were intubated for general anesthesia with a nerve integrity monitor (NIM) standard reinforced electromyography (EMG) endotracheal tube (Medtronic Xomed, Jacksonville, FL, USA). A dilute epinephrine solution (1:200,000) was injected into the subcutaneous space of the anterior chest area and into the subplatysmal space of the neck area. Incisions were made in the skin creases of the bilateral axillas and the upper median circumareolar areas. A vascular tunneler (GORE Tunneler-Standard Curve Access, W. L. Gore & Associates Inc., Flagstaff, AZ, USA) was placed through the incisions to detach most of the subplatysmal and subcutaneous areas. Bilateral axillary and circumareolar trocars were inserted and the operative area was insufflated with low pressure CO2 gas at 5-6 mmHg. The area under the skin flap was dissected further by using ultrasonic shears (Harmonic Scalpel, Ethicon Endosurgery, Cincinnati, OH, USA) to obtain a better operative field. After the strap muscles were separated in the midline, the isthmus was divided by using ultrasonic shears. While visualizing the RLN, the parathyroid glands, and the thyroid vessels, a thyroid lobectomy was performed. To avoid EBSLN injury, the superior thyroid vessels were ligated after identification of the EBSLNs or after confirmation of the absence of the EBSLNs using the NIM response 2.0 system (Medtronic Xomed). The EBSLNs were stimulated by directly placing the stimulation probe onto the nerve (if seen) or onto the cricothyroid muscle [13]. Identification of the EBSLNs was confirmed by an audible acoustic signal or contraction of the cricothyroid muscle. The stimulation level was set at 0.5-1 mA. The resected thyroid lobe was extracted through the axillary incision by using a plastic bag (LapBag, Sejong Medical, Paju, Korea). Contralateral lobectomy and central node dissection were performed if needed.
Voice assessment
All patients were examined preoperatively and at 1 and 3 months postoperatively to determine the degree of voice change. Patients were assessed using the subjective Voice Handicap Index-10 (VHI-10) and the objective maximal phonation time (MPT), phonation efficient index (PEI), and laryngeal EMG. We evaluated voice changes in patients with no evidence of RLN dysfunction in order to accurately evaluate the outcome of EBSLN monitoring using VHI-10, MPT, and PEI. Indirect laryngoscopic examination was performed routinely to evaluate vocal cord movement preoperatively and postoperatively. Patient with vocal cord palsy at first visit was reevaluated using laryngoscope at subsequent outpatient follow-up.
The VHI-10 is a validated, reliable self-assessment tool that measures voice quality as perceived by the patient and the effect of voice on quality of life (Table 1) [1415]. The VHI-10 consists of 10 questions that are scaled from 0-4, giving a score range from 0-40, representing no change to maximum change, respectively. MPT (a) and MPT (e) are measurements of the length(s) of sustained phonation of the vowels "a" and "e" at a loudness used in normal conversation after maximum inspiration in a sitting position [16]. MPT (a)/vital capacity (sec/L) can then be calculated. The value obtained indicates vocal cord function by converting a unit volume of exhaled air to a certain duration of phonation. This is called the PEI [17].
Laryngeal EMG
Laryngeal EMG allows us to diagnose nerve injury and to evaluate its severity with high diagnostic certainty [1819202122]. The cricothyroid and thyroarytenoid muscles of the patients were examined bilaterally by one of the authors using a concentric bipolar needle electrode connected to a 10-channel EMG-EP system (Synergy, Medelec, Oxford, UK). The gain was set as 100 mV/div, the filter setting as 20 to 10 kHz, and the sweep as 10 msec/div. After brief scanning for the target muscle locations using a linear ultrasonography probe (5-9 MHz; SonoAce 8800, Medison, Seoul, Korea), a needle electrode was inserted at the level of the lower margin of the cricothyroid membrane. For sampling of the thyroarytenoid muscle, the needle was advanced, passing through the cricothyroid membrane, heading upward (30 degrees from the coronal plane) and laterally (20 degrees from the sagittal plane), until muscle insertional activity was observed. The adequate needle location was verified by sounding "e" [23]. For the cricothyroid muscle, the needle electrode was inserted 2 mm lateral to the midline, and directed superiorly, laterally, and obliquely until the muscle was reached. The patient was asked to produce the vowel "e" in the as lowest and highest pitches as possible in order to verify proper needle location [24]. The presence of abnormal spontaneous activity such as fibrillation potentials, positive sharp waves, or complex repetitive discharge were thoroughly evaluated. The motor unit action potential morphology and interference pattern were also analyzed.
Statistical analysis
All data were presented as the mean ± standard deviation for all measured variables. Repeated measures analysis of variance was used to evaluate a change in VHI-10, MPT (a), MPT (e), and PEI among patients preoperatively and at 1 and 3 months postoperatively. The Duncan post hoc test was accompanied by repeated measures to assess the difference in each of the variables. A probability of less than 0.05 was considered as statistically significant. All statistical analyses were done using SAS ver. 9.1.3 (SAS institute Inc., Cary, NC, USA).
RESULTS
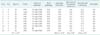
As shown in Table 2, all patients were female with a mean age of 35.1 ± 9.6 years (range, 26-57 years). Reasons for surgery included papillary thyroid cancer (n = 8), atypia of undetermined significane (n = 1), and nodular hyperplasia (n = 1). Nine patients (90.0%) were treated by total thyroidectomy with central node dissection, and 1 patient (10.0%) underwent unilateral lobectomy and isthmectomy. On final histology, 9 patients (90.0%) were diagnosed with papillary thyroid cancer and 1 patient (10.0%) was diagnosed with nodular hyperplasia. The mean duration of operation was 186.0 ± 33.0 minutes (range, 135-230 minutes). The mean tumor size and thyroid volume were 0.8 ± 0.8 cm (range, 0.4-3.0 cm) and 16.8 ± 4.0 g (range, 9.5-23.3 g), respectively. Thyroiditis was noted in 4 cases (40.0%). Conversion to open thyroidectomy was not reported in any case. There were 4 cases (40.0%) of transient hypoparathyroidism that resolved within 6 months postoperatively. There was no postoperative bleeding, chyle leakage, surgical site infection, or wound complications. Patients were discharged on postoperative day 3.0 ± 1.0 (range, 3-6 days) after removing the drain.
All patients completed a voice assessment. For each dissected lobe, we identified the RLN. EBSLNs were identified fourteen times (73.7%) by neuromonitoring, whereas 19 nerves were at risk.
Voice assessment
The VHI-10 showed a change of voice over time (0.1 vs. 3.6 vs. 1.3); however, this was not statistically significant (P = 0.056). The VHI-10 normalized at 3 months postoperatively compared to the preoperative value. MPT (a) (16.0 vs. 15.6 vs. 15.4) (P = 0.889) and MPT (e) (20.1 vs. 15.4 vs. 18.5) (P = 0.174) showed no significant differences between the preoperative value and the value observed at 1 and 3 months postoperatively. There was a significant change of PEI over time (4.8 vs. 1.1 vs. 4.6) (P = 0.036); however, this normalized at 3 months postoperatively (Fig. 1).
Laryngeal EMG
At preoperative examination, laryngeal EMG results showed that there were no abnormalities in bilateral RLNs and EBSLNs in all patients. At 1 month postoperatively, there were 4 cases (21.1%) of neuropathy of the EBSLNs out of 19 nerves at risk. Of these four, 2 cases (10.5%) exhibited mild axonotmesis and 2 cases (10.5%) exhibited moderate axonotmesis. At 3 months postoperatively, laryngeal EMG revealed an almost complete recovery in the function of the EBSLNs in these 4 patients. We also found 2 cases (10.5%) of axonotmesis of the RLN at 1 month postoperatively. EMG results showed an improvement in function of the RLN at 3 months postoperatively.
DISCUSSION
The aim of this study was to evaluate the feasibility and efficacy of neuromonitoring the EBSLNs during BABA robotic thyroid surgery. EBSLNs are at risk of injury during thyroid surgery and this can lead to a significant voice change [2526]. The nerve innervates the cricothyroid muscle, which acts together with the thyroarytenoid muscle to increase tension in the ipsilateral vocal fold [25]. In the present study, we used neuromonitoring during BABA robotic thyroid surgery to identify and preserve the EBSLN, and we performed ligation of the superior thyroidal vessels after confirmation of the absence of EBSLNs on the superior pole of the thyroid gland.
Several studies have been carried out to determine how to prevent injury of EBSLNs during thyroid surgery. Some of the techniques attempted included the following: skeletonization and individualization of superior thyroid pole vessels adjacent to the thyroid capsule of the gland, identification of EBSLNs before ligation at the superior thyroid pole [457], and use of a nerve stimulator or nerve monitoring [252627]. In a prospective randomized study, Bellantone et al. [7] found no significant differences between groups of patients who underwent skeletonization and individual ligation of the superior thyroid pole vessels close to the capsule compared with those in which the identification of EBSLNs took place before ligation of the superior thyroid poles vessels. Cernea et al. [25] revealed that intraoperative identification of EBSLNs using a nerve stimulator is useful to prevent iatrogenic injury of EBSLN lesions. Lifante et al. [26] found that neuromonitoring of EBSLNs during miniincision thyroidectomy under local anesthesia is useful to preserve subjective voice quality.
The present study is the first study to describe EBSLN monitoring during robotic thyroid surgery. We showed that EBSLN monitoring is technically feasible, safe, and useful to preserve the function of the EBSLN. In addition, the mean operation time recorded was 186.0 ± 33.0 minutes, which was not longer than that observed in a previous study where no monitoring of the EBSLNs during BABA robotic thyroid surgery took place [28]. EBSLNs were identified in 73.7% of cases, and the function of the EBSLNs was recovered in almost all cases at 3 months postoperatively.
We evaluated vocal outcome preoperatively and postoperatively for each patient using subjective and objective methods. For the former, the VHI-10 method, which is a validated assessment of patient perceived impact of voice quality, was used. Using VHI-10, we observed a change over time (P = 0.056); however, the Duncan post hoc test revealed that VHI-10 normalized at 3 months postoperatively. For objective methods, we used MPT (a), MPT (e), and PEI. MPT (a) and MPT (e) results revealed that there was no significant change in voice over time. The PEI results did, however, show a significant change over time (P = 0.036). The Duncan post hoc test revealed that PEI normalized at 3 months postoperatively. We assessed vocal function in 8 patients without RLN dysfunction to accurately evaluate EBSLN function using VHI-10, MPT (a), MPT (e), and PEI. We performed laryngeal EMG of the cricothyroid muscles on 10 patients. This is the most objective method that allows us to know the actual function of the EBSLNs with greater diagnostic certainty than other methods, such as indirect or direct laryngoscopy [1819202122] or videostrobolaryngoscopy. With these techniques, the results can be altered by temporal or definite dysfunction of the extralaryngeal muscles after surgery, inadequate voice use technique, gastroesophageal reflux, and even the emotional state of the patients [37272930]. At 1 month postoperatively, there were 4 cases (21.1%) of EBSLN neuropathy. At 3 months postoperatively, results of laryngeal EMG showed nearly complete recovery of the EBSLN. EBSLN neuropathy was observed in three out of the 14 cases (20.4%) in which EBSLNs were identified during operation, and in 2 out of the 5 cases (40.0%) in which EBSLNs were not identified during operation, using laryngeal EMG at 1 month postoperatively. However, this was not statistically significant (P = 0.570). Due to the small sample size in the present study, we could not find the priority of preservation of the EBSLNs in the group in which EBSLNs were identified compared to the group in which it was not identified and it was not possible to identify the factors that influence the frequency of EBLSN injury.
Despite best efforts to localize, the EBSLN was not identified by direct electrical stimulation in some cases. One explanation for the finding is that neuromonitoring of the EBSLN is more challenging than that of the RLN because the endotracheal recording electrodes are closer to the thyroarytenoid muscle than to the cricothyroid muscle. In the EBSLN monitoring, the cricothyroid muscle, the electrical source generator, is several millimeters apart from the electrodes, which can reduce the amplitude of electrical activities. In this regard, patients with larger larynx are likely to have smaller or absent muscle activities as the distance between electrodes and muscles increases. However, electrical muscle activities larger than the 100-150 µV thresholds could easily be elicited by direct EBSLN stimulation in 73.7% of the cases.
Although the present study was a pilot study for the feasibility of EBSLN monitoring during BABA robotic thyroid surgery, we discovered that EBSLN monitoring is useful to preserve voice quality. We observed a minimal voice change in patients using EBSLN monitoring during BABA robotic thyroid surgery; however, this change normalized at 3 months postoperatively compared to preoperatively. We now need further prospective randomized studies to evaluate the advantages of EBSLN monitoring over no monitoring, and to identify the risk factors that lead to voice changes after robotic thyroid surgery.
In conclusion, it is suggested that neuromonitoring of the EBSLNs during BABA robotic thyroid surgery is feasible and might be helpful in order to preserve voice quality. Future prospective randomized studies are required to confirm the efficacy of neuromonitoring of the EBSLNs during BABA robotic thyroid surgery.


 XML Download
XML Download