

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatic cancer has the worst prognosis of all gastrointestinal malignancies. Complete surgical resection offers the only chance to cure the disease. However, only 15% to 20% of pancreatic cancer is resectable at the time of diagnosis [1]. The prognosis of unresectable pancreatic cancer is extremely poor. The causes for unresectability are distant metastasis in approximately two thirds of the cases and locally advanced disease in one third of the cases [2]. Tumors that involve the celiac axis (CA) and superior mesenteric artery (SMA) are defined as T4 according to 7th edition of American Joint Committee on Cancer staging system and these tumors are generally regarded as unresectable. However, some authors reported successful carcinoma resection of the body and tail of the pancreas involving the common hepatic artery (CHA) and/or CA when the collateral arcade between SMA and CA is intact [3].
With the advances in high quality CT imaging, new concepts that define the extent of venous and arterial invasion have been developed and a subset of tumors that blur the distinction between resectable and locally advanced pancreatic cancer is categorized as borderline resectable pancreatic cancer (BRPC). Despite the high risk of disseminated disease and incomplete resection, some BRPC are now regarded as resectable tumors [1].
Distal pancreatectomy with en bloc celiac axis resection (DP-CAR) may offer R0 resection for the tumors invading CA and BRPC. Thus, to investigate the clinical effects of DP-CAR, we reviewed clinico-patholocial features, and surgical outcomes of the patients who underwent DP-CAR with literature review.
METHODS
From January 2000 to November 2014, 55 consecutive patients with invasive ductal carcinoma of the body and tail of the pancreas underwent surgery. Thirty-eight patients underwent resection, whereas 17 patients could not undergo resection because unresectable lesions were found during surgery. During this period, we began performing DP-CAR from June, 2011.
Among 38 patients who underwent resection, 7 patients including 6 cases of T4 unresectable pancreas cancer and 1 case of BRPC according to the current guidelines and TNM staging [4] underwent a distal pancreatectomy with en bloc CA resection. The remaining 31 patients received conventional distal pancreatectomy (Table 1). Seventeen patients who were deemed to have resectable disease preoperatively turned out to be unresectable. The most common causes of unresectability were peritoneal metastasis (12 of 17) followed by liver metastasis (2 of 17), concomitant metastasis at peritoneum and liver (2 of 17), and extensive local invasion (1 of 17).
In adjuvant setting, only the patients who elected to have chemotherapy were treated by gemcitabine. Gemcitabine at a dose of 1,000 mg/m2 was administered weekly for 3 weeks followed by 1 week of rest within 2 months after the surgery. In detail, adjuvant chemotherapy was given to 2 out of 7 patients (28.6%) of DPCAR group and 11 out of 31 patients (35.5%) of DP group. Also, for 17 patients who could not undergo resection, palliative chemotherapy (gemcitabine or oral 5-fluorouracil) was performed in 7 out of 17 patients (41.2%).
Among the 7 patients who underwent DP-DAR, six cases were definitely T4 invading CA on preoperative CT staging. The remaining patient showed features of BRPC with suspicious invasion of the CA and definite invasion of the origin of the splenic artery (SA), which makes R0 achievement impossible without CA resection. We decided to perform DP-CAR for this last case (Table 2).
In this study, the primary endpoint was to find out the immediate postoperative results of DP-CAR including operation time, duration of hospital stay, postoperative morbidity and mortality. The primary endpoint of DP-CAR was compared to that of all 31 consecutive patients who underwent conventional distal pancreatectomy.
The secondary endpoint was to determine the effect on prognosis of DP-CAR. To determine the prognostic effect of DP-CAR compared to conventional distal pancreatectomy, we selected 22 patients with tumors in similar stage (pT3 or pT4) as a matching control group (DP group, n = 22) out of 31 patients who underwent conventional distal pancreatectomy.
Clinico-pathological data and surgical outcomes among the three groups were collected and statistically analyzed using a chi-square test and Fisher exact test. Postoperative survival was analyzed using the Kaplan-Meier method and the log-rank test.
Surgical indications and method
Surgery was performed for patients without distant metastasis on the preoperative imaging study. We performed DP-CAR for selected patients in whom invasive ductal carcinoma of the body and tail of the pancreas possibly involved or abutted the CHA, the root of the SA, and/or CA without invasion to the aortic wall. If the proper hepatic artery (PHA), SMA, gastroduodenal artery (GDA), or pancreaticoduodenal arcade is invaded, DP-CAR was not indicated (Fig. 1).
After explolaparotomy, we performed a full exploration of the abdomen. It is very important to confirm the collateral circulation to the liver via pancreaticoduodenal arcade before dividing the CA. To confirm sufficient hepatic perfusion and assess the tumor involvement of the CA, the lymph nodes around the hepatic artery were dissected to the CA exposing the artery. The pulsation of the PHA before and after clamping the artery was compared manually and by using Doppler ultrasound examination. When hepatic arterial flow was confirmed, we proceeded to divide the pancreas neck creating a tunnel between the pancreas and the portal vein (PV). We divided the pancreas just above the PV assessing the tumor involvement of the venous confluence. Dissection was then continued in a retrograde fashion, clearing tissue from the anterior surface of the PV and SMA to the aortic root of the CA. Nerve plexus and lymphatic tissue around the SMA and CA was dissected en bloc. After isolation of CHA, we divided the CHA with sufficient tumor free margin. When the aortic root of CA was isolated, it was divided with suture ligation. Then the splenic vein was divided at the confluence with superior mesenteric vein (SMV). The body and tail of the pancreas and spleen are dissected free from the left adrenal gland and Gerota's fasica (Fig. 2). The status after DP-CAR is shown in Fig. 3.
RESULTS
Comparison of clinico-pathological features between DP and DP-CAR groups
The median age of both DP and DP-CAR group was 67.5 and 58 years, respectively. The patients of DP-CAR group was younger compared to the patients of DP group, but the age of the two groups was not statistically different (P = 0.068). Male to female ratio was also not different between both DP and DP-CAR groups (P > 0.999). Although serum level of CEA was not different between the two groups (median 2.1 vs. 2.4, P = 0.469), serum level of CA 19-9 in DP-CAR group was higher than that of DP group. (median 86.7 vs. 281.9, P = 0.014) (Table 1).
The size of tumor in DP-CAR group was larger than that of DP group (40 mm vs. 55.8 mm, P = 0.061) although there was no statistical difference. The perineural invasion was more frequently observed in DP-CAR group (45.2% vs. 100%, P = 0.011). However, nodal status and histologic grade were not statistically different between the two groups (Table 1).
The pathological T-staging of the 7 patients who underwent DP-CAR revealed pT4 in 4 patients and pT3 in 3 patients. R0 resection was possible in 5 patients in DP-CAR group (71.4%) (Table 2) whereas R0 resection was achieved in 80.6% (25 of 31) of all 31 patients who underwent conventional DP. The R0 resection rate was not statistically different between the two groups (71.4% vs. 80.6%, P = 0.115) (Table 1).
Comparison of immediate postoperative results between DP and DP-CAR groups
Compared to DP group, the median operative time (median 286 minutes vs. 354 minutes, P = 0.022) and length of hospital stay after surgery (median 14.5 days vs. 23 days, P = 0.022) of DP-CAR group were significantly longer. And, the DP-CAR was associated with greater blood loss (mean 727 mL vs. 300 mL, P = 0.024), and more blood transfusion (mean 286 mL vs. 24 mL, P = 0.001) (Table 3).
To compare the complication rate according to surgical procedures, we adopted the definitions of postoperative pancreatic fistula (POPF), delayed gastric emptying, and post-pancreatectomy hemorrhage (PPH) defined and proposed by the International Study Group of Pancreatic Surgery [567]. In DP-CAR group, postoperative complications included grade B POPF in 1 patient (14.3%), focal hepatic infarction in 1 patient (14.3%), transient hepatopathy in 3 patients (42.9%), and mild diarrhea in 3 patients (42.9%). However, no patients of DP-CAR group had evident ischemic gastropathy, hepatic failure, or postoperative bleeding. Grade B pancreatic fistulas occurred in 22.6% (7 of 31) of DP group and 14.3% (1 of 7) of DP-CAR group. Grade C POPF occurred in 1 patient (3.2%) in DP group but no grade C POPF occurred in DP-CAR group. The incidence of POPF was not statistically different between DP and DP-CAR group (P = 0.123). In DP Group, grade C PPH occurred in 1 patient (3.2%) but no PPH occurred in DP-CAR group. No mortality occurred in DP-CAR group but one mortality case occurred in DP group. The mortality rate was not different significantly between the two groups (P > 0.999) (Table 3). The cause of death was sepsis and multiorgan failure related to grade C POPF.
Comparison of survival among DP group, DP-CAR, and no resection group
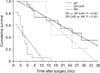
To determine the prognostic effect of DP-CAR, the data of DP-CAR group was compared to the 22 matching patients confirmed to have pT3 or pT4 selected out of 31 patients who underwent distal pancreatectomy. The results are shown in Fig. 4. The 1- and 2-year survival rates in the patients who underwent conventional DP were 73.7% and 55.3%, respectively. In the patients who underwent DP-CAR, the 1- and 2-year survival rates were 100% and 44.4%, respectively. The median survival time (MST) after DP were somewhat longer than that after DP-CAR (median 25 months vs. 15 months, P = 0.681) but the difference of overall survival did not reach statistical significance (Fig. 4). When compared to the patients with no resection (NR group), the patients of DP-CAR group had longer MST (median 15 months vs. 4.0 months, P < 0.001).
In DP group, recurrence occurred in 14 patients out of 22 (63.6%) and 6 patients out of 7 (85.7%) had recurrence in DP-CAR. The incidence of reccurence were not statistically different between DP and DP-CAR group (P = 0.382).
Among the 6 patients who had recurrences in DP-CAR group, 2 patients had local recurrence with concomitant distant metastasis, and the 4 remaining patients had distant metastasis only: 1 hepatic, 1 pulmonary, 1 peritoneal, and 1 paraaortic lymph node metastasis. Out of 6 patients with recurrences, 4 patients died and 2 patients are alive (Table 4).
DISCUSSION
Due to the lack of specific symptom associated with pancreatic body and tail carcinoma, more than 80% of these tumors are in unresectable status at the time of diagnosis [1]. The causes of unresectability are due to distant metastasis in approximately two thirds and advanced disease involving CA and SMA without distant metastasis in one third [2]. Among locally advanced diseases, pancreatic body and tail cancers involving or abutting the CA have been a unique dilemma for surgical treatment and a surgical challenge for hepatobiliary surgeons. Unlike T4 tumors invading SMA, the T4 tumors invading the CA can be resected by CA resection without arterial reconstruction if the hepatic blood flow through the collateral arcade between SMA and the CA is not impaired by other lesions such as arthrosclerosis or anomalies.
The tumors invading the CA usually are large, invade surrounding connective tissue, and accompanied by nodal metastasis making complete resection difficult. In many cases, the resection results in R1 or R2 resection. However, in selected patients of such diseases, en bloc resection of the CA can help to achieve complete R0 resection of body-tail pancreatic cancer with an extensive dissection of the nerve plexus and retroperitoneal tissue. There is no doubt that complete R0 resection is the only treatment with the chance for a cure [89].
Since Nimura et al. [10] first adapted this procedure to resect tumors of the body and tail of the pancreas in 1976, this procedure has been modified by many surgeons with various reports. Hirano et al. [11] reported good results of 23 patients who underwent DP-CAR. They reported no mortality and the mean survival was 18.2 months and five-year survival rate was 42%. They also showed that DP-CAR could offer a high R0 resectability rate of 91% and insisted that DP-CAR potentially can achieve complete local control in selected patients. Other reports also showed the R0 resection rate between 30.8%-100%. The MST varied between 9.7-25 months after DP-CAR (Table 5).
Previously we did not perform the surgery if the CA was involved. However, since June 2011 we set up a policy to resect the tumors if CA resection is involved. In our experience of DP-CAR, patients tend to be young although the difference did not reach statistical significance. This may be due to the fact young patients are more eager and open to accept more aggressive surgical options. In DP-CAR group, the size of tumor was larger and presence of perineural invasion was more frequent than in DP group, as shown in Table 1.
All seven patients had been regarded as having unresectable tumors from the view point of the previous policy. However, with the introduction of CA resection combined with extensive dissection of surrounding tissues, we were able to achieve R0 resection from the patients with seemingly unresectable pancreatic body and tail cancer. In our study, we were able to achieve R0 resection in 71.4% of the patients comparable to that of patients who underwent conventional distal pancreatectomy. This result is similar to the recent reports as shown in Table 5.
The potential specific complications associated with DP-CAR may include first, direct injury to the SMV, SMA, and aortal wall and second, ischemic injury of liver and stomach. In our experience, we did not have direct vascular injuries and postoperative bleeding, which may happen during the dissection along the left side of SMA to the aortic wall. To avoid ischemic gastropathy, we removed the distal stomach in the first patient of DP-CAR group. However, in the first patient, we noticed active pulsating arterial blood flow pattern around the cut edge of the stomach after division of the CA, thus we decided to preserve the whole stomach from the second patient. The preservation of the stomach during DP-CAR is controversial. Because the blood flow to the stomach is maintained thorough the right gastric artery, right gastroepiploic artery, left phrenic artery, and the intramural capillary network from the esophagogastric junction after the DP-CAR, the stomach can be preserved. On the basis of these concepts, we preserve the whole stomach if the stomach is not directly invaded. Also, to prevent ischemic gastropathy, the right gastric and right gastroepiploic arteries should be preserved during the dissection of the regional nodes and nerve plexus. Although the authors were not trying, preoperative coil embolization of the CHA can develop collateral circulation. Also, the preservation of the right gastric vein and right gastroepiploic veins should be considered for the prevention of congestive gastropathy.
Asymptomatic transient mild hepatic injury with mild elevation of transaminase was soon normalized. A case of focal hepatic infarction was detect by routine postoperative CT scan but it was also asymptomatic and resulted in shrinkage of the affected area without further complications. Other complication associated with distal pancreatectomy itself was not different from conventional distal pancreatectomy.
Literature review showed that the postoperative mortality and morbidity rates of DP-CAR varied between 0%-10% and between 28.6%-92.3%, respectively (Table 5). Our results also showed that DP-CAR can be safely performed comparable to conventional DP.
R0 resection is most important for improving the prognosis after surgery for pancreatic body and tail cancer. With the introduction of DP-CAR, we were able to achieve R0 resection rate of 71.4%. Two-year survival of the 22 selected patients selected as matching control group, who underwent a macroscopically curative resection, was 55.3% for DP whereas the 2-year survival of the patients in DP-CAR group was 44.4%. The MST of patients who underwent conventional DP and DP-CAR were 25 and 15 months, respectively. Between the two groups, no statistically significant difference was found in terms of overall survival. In contrast, when compared to the patients with no resection, survival of patients with DP-CAR was better (median 15 month vs. 4 months, P < 0.001) (Fig. 4). The results of this study suggest that DP-CAR may be beneficial in terms of survival.
The limitations of this study are that it is a retrospective study and the control patients of DP group and no resection group are not matched well. These problems arise from the paucity of pancreas body and tail cancer invading the CA without distant metastasis. Since these problems make it difficult to determine the prognostic effect of DP-CAR exactly, further studies with a large number of patients at the multicenter level are required.
In summary, although DP-CAR was more technically demanding than conventional distal pancreatectomy, DP-CAR could be performed with an acceptable safety and radicality in the selected patients with a locally advanced body-tail pancreas cancer.
In conclusion, DP-CAR was technically feasible without serious complication and offers a high R0 resectability rate for patients with carcinoma of the body and the tail of the pancreas definite or suspicious of invading CA. Short-term survival of DP-CAR is comparable to DP and better than no resection. However, the benefit needs to be verified by further studies in the future.








 XML Download
XML Download