

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the increasing proportion of elderly patients in the general population and regular medical check-ups, the occurrence of synchronous primary cancers is becoming more frequent. Nevertheless, triple synchronous primary cancers are regarded as a very rare occurrence. In this report, we present a case of synchronous triple cancers occurring in the stomach, kidney, and thyroid upon routine screening.
CASE REPORT
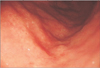
A 50-year-old man was admitted to our hospital owing to early gastric cancer (EGC) detected upon esopha gogastroduodenoscopy (EGD) during a routine check-up. A family history of thyroid cancer was determined, with his sister having undergone resection for thyroid cancer. His medical history included hypertension and, consequently, he received medication for treatment. Physical examination revealed no significant findings. Laboratory investigations did not show any significant abnormalities. The tumor markers were within normal limits. EGD revealed an EGC type IIb lesion at the lower portion of the stomach, and the pathology report showed poorly differentiated adenocarcinoma (Fig. 1). An abdominal/pelvic CT scan showed no significant lymph node (LN) enlargement due to gastric cancer but did show a 1.7-cm exophytic hypervascular renal mass in the inferior pole of the left kidney, which was determined to be renal cell carcinoma (Fig. 2).
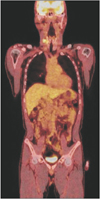
We performed thyroid ultrasonography and fine needle aspiration biopsy (FNAB). Two 1.6 and 0.9 cm probably malignant thyroid nodules were found, which was bulging into the superior and lateral capsule with microcalcification, as well as several conglomerated LNs with jugular vein invasion in the right side of the neck (Fig. 3). FNAB results indicated papillary thyroid carcinoma and level IV LN metastasis. 18F-fluorodeoxyglucose (18F-FDG) PET/CT showed a focal FDGavid nodule with calcification in the right upper thyroid lobe, level III and IV LNs metastasis in the right side of the neck, and an isometabolic nodule in the left kidney (Fig. 4). No definite abnormal FDG uptake along the gastric wall was noted.
Our team performed a radical subtotal gastrectomy, a consecutive left partial nephrectomy, and a radical thyroidectomy with modified radical neck dissection in the right side of the neck. Total operative time was 315 minutes and total bleeding amount was check 400 mL.
The pathology report following gastrectomy determined the tumor to be EGC type IIc, tubular adenocarcinoma, moderatelyto-poorly differentiated, intestinal type by the Lauren classification, with a depth of invasion above the muscularis mucosa (T1a) and with no metastases in any of the 45 LNs assessed (T1N0M0; stage 1A). The pathology report following partial nephrectomy showed a 1.9 × 1.5-cm completely encapsulated renal cell carcinoma, a clear cell histology, and a pathologic stage of T1aN0M0; stage 1. And the pathology report following thyroidectomy indicated the presence of a 2.0 × 1.5-cm thyroid papillary carcinoma, with recurrent laryngeal nerve, jugular vein (T4b) and extensive lateral LNs involvement in 10 of 22 LNs assessed (T4aN1bM0; stage 4A). After the three consecutive operations, the patient was in good health and was discharged without any postoperative complications.
DISCUSSION
Although the incidence of multiple primary cancers has been reported to vary from 0.7 to 11.7% [1], reports of multiple synchronous primary cancers have increased owing to the increased population of elderly patients and routine general check-ups in this population. A study by Lee et al. [2] showed that the incidence of synchronous cancer in gastric cancer patients was 3.4%, with the most common synchronous sites being colorectal cancer (37.2%), followed by lung cancer (18.6%), esophageal cancer (16.8%), liver cancer (9.7%), and kidney cancer (4.4%).
Synchronous tumors are defined as ≥2 primary tumors occurring within 6 months of diagnosis of the first primary tumor. The histologic criteria of synchronous malignant neoplasm established by Warren and Gates are as follows: tumors must be clearly malignant, as determined by histologic evaluation; each neoplasm must be topographically separate and distinct; the probability that one is a metastatic lesion from the other must be ruled out [1,3]. According to these criteria, this case was determined as being synchronous triple primary cancers. The patient was diagnosed with EGC on routine check-up EGD and thyroid cancer on thyroid ultrasonography owing to a family history of thyroid cancer. Additionally, renal cell carcinoma was found in the left kidney during an abdominal and pelvic CT scan for staging work-up. We also performed FDG-PET/CT for a further staging work-up of this patient, identifying thyroid cancer with LN metastasis as well as gastric and kidney lesions. It has been reported that half of all clinical T1 lesions can be detected by FDG-PET/CT which suggests that FDGPET/CT is not only useful to identify distant metastases of the primary tumor, but also for the purpose of detecting second primary synchronous cancers [4,5]. For multiple primary cancers, including head and neck, gastric, and colon cancer, it is hypothesized that chemical and physical stimuli affect the route from the oral cavity to the upper and lower gastrointestinal system, leading to field carcinogenesis [6].
One of the most important factors when deciding the best treatment modality for multiple primary cancer patients is the stage of the synchronous cancers [7]. According to a recent study, stage I gastric cancer with double primary malignancy had a worse prognosis. Moreover, gastric cancer patients over the age of 60 years or with microsatellite instability-high status were associated with double primary malignancy [8]. Yoshino et al. [9] reported that the prognosis of patients with multiple primary cancers can be determined independently by the stage of each cancer. On the final pathology report of this patient, gastric and kidney tumors were determined to be in an early stage and without node metastasis. However, the pathology of the thyroid tumor was more aggressive than the other two lesions, and therefore, the prognosis of this patient could be determined by the thyroid cancer. This patient received adjuvant treatment following radical total thyroidectomy, owing to the advanced stage of the thyroid cancer, but not following left partial nephrectomy or radical total gastrectomy. To our knowledge, there have been no similar reported cases of triple primary cancers (gastric cancer, thyroid cancer, and renal cell cancer).
In conclusion, this case report identifying synchronous gastric cancer, thyroid cancer, and renal cell cancer is noteworthy owing to its rare occurrence.


 XML Download
XML Download