

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Even though endovascular therapy can be successfully performed with various kinds of balloons, stents, or stent grafts, lower extremity arterial bypass (LEAB) surgery remains the most viable treatment option for patients with atherosclerotic arterial occlusive disease, particularly those with diffuse and long segment lesions of the superficial femoral artery (SFA) [1]. The superiority of vein grafts to prosthetic grafts has been well proven in below-the-knee arterial bypass [2,3,4]. However, previous studies have shown mixed results in above-the-knee femoro-popliteal bypass (ATKFPB) [5,6,7,8,9,10,11,12]. One prospective randomized trial [9] that compared graft patency at two years after ATKFPB reported no statistically significant difference in primary or secondary patency rate between vein grafts and polytetrafluoroethylene (PTFE) grafts. Other randomized controlled trials [6,7,11,13,14] that compared long-term patency rates reported significantly higher patency rates of vein grafts compared with PTFE grafts. Most studies comparing the efficacy of these two types of grafts have been based on graft patency [5,6,7,8,9,10,11,12,13].
However, graft recommendations should not be based solely on the superiority of graft patency. Approximately 10 years ago, Jackson et al. [15] reported different clinical features in cases of LEAB graft occlusion that had received vein grafts versus those that had received prosthetic grafts; moreover, PTFE graft is associated with a higher risk of ischemic complications from graft occlusion than are vein grafts. However, few reports have investigated the clinical consequences of graft occlusion.
In this retrospective review, we compare the long-term patency rates of ATKFPB with vein grafts versus PFTE grafts. We also compare the clinical outcomes of graft occlusions in these two groups.
METHODS
Study design, patients, and data collection
We retrospectively reviewed a database of patients with chronic atherosclerotic occlusive lesions who underwent ATKFPB at a single institute during the past 10 years (September 2003 through February 2014).
Patients with nonatherosclerotic occlusive disease who underwent LEAB were excluded from this study. The decision to insert a bypass conduit during ATKFPB was left to the surgeon. In total, 107 autogenous vein grafts and 146 PTFE grafts were performed. All vein grafts used the reversed great saphenous vein as the conduit. The prosthetic grafts were either external supported or smooth PTFE grafts (Gore-tex, W. L. Gore & Associates Inc., Newark, DE, USA) that were 7 or 8 mm in diameter.
Between-group differences in preoperative demographic data, clinical features, distal runoff artery status, adjunctive procedures, and procedural details were compared. The distal runoff score was calculated according to the reporting standards on preoperative angiograms as outlined by the Joint Council of the Society for Vascular Surgery and the North American Chapter of the International Society for Cardiovascular surgery [16].
Postoperatively, all patients with vein grafts except one were prescribed single antiplatelet therapy unless contraindicated. Moreover, 126 patients (vein grafts, 11.2% vs. PTFE grafts, 57.7%; P < 0.001) were prescribed warfarin due to concomitant cardiac arrhythmia or to prevent graft thrombosis. For graft surveillance, periodic examinations of duplex ultrasonography scans were performed by experienced vascular technicians at one month postsurgery and then every 3-6 months throughout the first 12 months postsurgery; after this period, examinations were performed every 6-12 months. The graft surveillance procedures were identical for the two groups.
Primary, primary-assisted, secondary patency rates of the grafts, and cumulative limb salvage rates were compared and the clinical courses of target limbs were also compared between the vein graft and PTFE graft groups in patients with graft occlusion.
Data analysis and statistical methods
Either Student t-test or the Mann-Whitney test was used to compare descriptive variables between the two groups. The chi-square or Fisher exact test was used to compare categorical data. Primary, primary-assisted, secondary patency, and limb salvage rates were calculated using the Kaplan-Meier method, and the log-rank test was used to examine differences between the two groups. Statistical analysis was performed with IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). P-values of <0.05 were considered to be significant.
RESULTS
Among the 253 ATKFPBs performed for 228 patients (mean age, 68.5 years; range, 42-90 years; male, 87.7%), reversed great saphenous vein grafts were performed on 107 limbs (42.3%) and PTFE grafts were used on 146 limbs (57.7%).
The patient characteristics of the two groups are compared in Table 1. No significant differences regarding demographic features, surgical indications, distal runoff scores, coexisting morbidities, or risk factors were observed between the two groups. With respect to the transatlantic society consensus (TASC) classes in the two groups, all patients except one showed class C or D lesions according to the TASC II classification scheme. The details of the ATKFPB procedures in the two groups of patients, including the frequencies of previous interventions, inflow procedures, proximal anastomosis sites, adjuvant procedures, and postoperative antithrombotic medications, are summarized in Table 2. In the PTFE grafts group, proximal anastomosis of the ATKFPB was more frequently performed at the inflow graft; moreover, adjuvant femoral endarterectomies were also more frequently performed in this group.
During the postoperative follow-up period (mean, 41 ± 32 months; range, 1-122 months), 33 patients (14.5%) died, and 15 grafts (5.9%) were lost to follow-up.
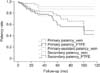
The graft patency rates of the vein graft and PTFE graft groups are compared in Fig. 1. No significant difference in primary patency (75% vs. 59% at 5 years; 75% vs. 42% at 10 years, P = 0.330) was observed between the two groups. However, primary-assisted (88% vs. 59% at 5 years; 88% vs. 42% at 10 years, P = 0.003) and secondary graft patency rates (91% vs. 76% at 5 years; 91% vs. 49% at 10 years, P = 0.013) were significantly higher in the vein graft group at 10 years after ATKFPB.
During the follow-up period, graft (or anastomotic site) stenosis (n = 18, 7.1%) was more frequently detected in the vein graft group (vein grafts, 14.0% vs. PTFE grafts, 2.1%; P < 0.001), whereas graft occlusions (n = 36, 14.2%) were more frequently detected in the PTFE graft group (vein grafts, 5.6% vs. PTFE grafts, 20.5%; P = 0.001). The clinical features of graft occlusions also differed between the two groups. All vein graft occlusions (n = 6, 5.6%) presented as recurrent leg claudication, with the exception of one asymptomatic limb. In contrast, PTFE graft occlusion more often presented as acute limb ischemia (vein graft, 0% vs. PTFE grafts, 53.3%; P = 0.027) (Table 3). Despite various treatments of the graft occlusions, limb loss occurred significantly more frequently in the PTFE graft group than in the vein graft group (vein grafts, 0% vs. PTFE grafts, 4.8%; P = 0.019) (Table 3, Fig. 2).
DISCUSSION
LEAB is still used as the last option for arterial reconstruction in patients with symptomatic, diffuse atherosclerotic occlusive disease; LEAB is typically performed as a primary or secondary procedure following failed endovascular or open surgical procedures [1,17,18]. Although an autologous saphenous vein is generally the conduit of choice in distal leg bypass surgery, the superiority of vein grafts to prosthetic grafts in ATKFPB has been disputed.
Several previous prospective randomized controlled trials have reported different follow-up results after comparing vein grafts and prosthetic grafts in ATKFPB. However, this issue has become less important as endovascular therapy has become a more relevant treatment for SFA lesions.
In a prospective randomized trial comparing vein grafts with PTFE grafts in ATKFPB, Burger et al. [9] reported no significant differences in the primary and secondary patency rates at two years after bypass surgery (83% vs. 67%, P = 0.065; 83% vs. 77%, P = 0.298). Veith et al. [14] also reported in a randomized controlled study that the 4-year graft patencies of patients who underwent ATKFPB with autogenous saphenous vein grafts versus those with PTFE grafts were not significantly different (68% vs. 38%, P = 0.25). In another randomized trial comparing vein graft, human umbilical vein graft, and PTFE graft outcomes after ATKFPB, similar 2-year patency rates were reported (saphenous vein, 81%; human umbilical vein, 70%; PTFE, 69%); however, that study found a significantly higher 5-year patency rate of saphenous vein grafts compared with PTFE grafts (73% vs. 39%, P < 0.01) [11]. The data presented by Tilanus et al. [19] also support the superior long-term patency of vein grafts compared to prosthetic grafts in ATKFPB (70% vs. 37%, P < 0.001).
In the present study, we did not observe a statistically significant difference in the long-term primary patency rates of vein grafts compared with PTFE grafts (75% vs. 42%, P = 0.330) at 10 years after graft implantation. However, we did find that the primary-assisted patency and secondary patency rates of the vein grafts were significantly higher at 10 years compared with those of the PTFE grafts (primary-assisted patency, 88% vs. 42%, P = 0.003; secondary patency, 91% vs. 49%, P = 0.013) (Fig. 1). The discrepant results of the primary patency rates compared with those of the primary-assisted and secondary patency rates may be attributed to the higher rate of detection and revision of the failing grafts in the vein graft group compared with the PTFE graft group (14.0% vs. 2.1%, P < 0.001).
Given that SFA lesions that require ATKFPB are as not as diffuse or atherosclerotic as SFA lesions that require distal leg bypass grafting, it was not surprising that we observed a significant difference in the limb salvage rates between the two groups (Fig. 2). The clinical results of patients with graft occlusions also revealed that patients in the PTFE graft group exhibited poorer clinical outcomes, including a higher frequency of acute limb ischemia (0% vs. 53.3%, P = 0.027). The poorer late clinical outcomes of the PTFE grafts may be attributed to differences in biological impact on the surrounding native arteries from the autogenous vein graft. This hypothesis is supported by the higher frequency of sudden occlusion associated with PTFE graft (vein graft, 5.6% vs. PTFE graft, 20.5%; P = 0.001) and the more frequent graft narrowing in vein grafts (vein graft, 14.0% vs. PTFE graft, 2.1%; P < 0.001) (Fig. 3). These findings may be due to sudden thrombosis, which occurs more frequently in prosthetic grafts than in vein grafts, in which intimal hyperplasia is the major cause of late graft occlusion [20]. As reported in previous studies [15,21], rapid revascularization is required to manage the impact of sudden graft thrombosis on the local collateral circulation and the persistence of foreign graft material in tissues. Such events may lead to higher limb loss rates in cases of prosthetic graft occlusion compared with those of vein graft occlusion.
According to our assessment of LEAB results, limb salvage rather than graft patency shows a more striking difference between the two groups, particularly in the context of the preservation of a painless and functioning limb that does not require reintervention. From this point of view, our retrospective analysis leads us to recommend vein grafts rather than PTFE grafts as bypass conduits for ATKFPB.
Furthermore, the importance of postoperative surveillance of vein grafts and early treatment of failing vein grafts is highlighted by our analysis, which revealed a higher assisted primary graft patency rate in the vein graft group, in accordance with previous studies [15,22].
Moreover, the argument that PTFE grafts should be used in ATKFPB in order to preserve the great saphenous vein for future coronary artery bypass grafting (CABG) has become less convincing due to the availability of improved conduits for CABG and the increasing incidence of percutaneous coronary artery intervention [23,24].
This study was somewhat limited by its retrospective design; moreover, patients who underwent ATKFPB were not allocated randomly into the vein graft group or the PTFE group.
In summary, this study shows that long-term patency rates and clinical outcomes after ATKFPB were significantly better with vein grafts compared with PTFE grafts. In addition, this study highlights the importance of postoperative vein graft surveillance and treatment of failing grafts for successfully preventing graft failure. Accordingly, we propose that ATKFPB with a vein graft and postoperative graft surveillance should remain the preferred treatment for patients with diffuse, long occlusive lesions of the SFA.





 XML Download
XML Download