

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Conventional laparoscopic (CL) colectomy is widely considered to be a technically demanding procedure that has a steep learning curve. There is a growing interest in the recently introduced technique of single incision laparoscopic (SIL) colectomy. So far, the advantages of SIL colectomy over CL colectomy have not been firmly proven, although the superior wound cosmesis afforded by SIL colectomy has motivated some patients and surgeons to opt for this operation. Despite awareness of SIL colectomy and its increasing popularity, some CL colorectal surgeons may be hesitant to embark on SIL colorectal surgery for various reasons, including the need to overcome another learning curve. Although numerous studies on the learning curve of CL colectomy have been published since the 1990s [1,2,3,4,5,6], few studies as yet has investigated the learning curve of SIL colectomy.
The aim of this study were therefore to evaluate and compare the learning curves of CL and SIL right hemicolectomy (RHC) performed by a single colorectal surgeon, and determine the early outcomes of both techniques based on the surgeon's initial experience.
METHODS
This study is a retrospective review of prospectively collected data on CL and SIL RHC which were performed by a single colorectal surgeon (S.H.Y.) in Samsung Medical Center. The surgeon first started to perform CL RHC in March 2005 and had performed 60 cases of CL RHC before he embarked on his first case of SIL RHC in October 2009. The initial 35 patients of each group were included to compare the learning curve and early postoperative outcomes. Clinicopathologic parameters, operation time and postoperative complications were analyzed. In all cases, informed consent was provided by patients.
Surgical techniques
Patients were placed in a supine position. For SIL RHC, a 3- to 4-cm transumbilical vertical incision was made. A wound retractor (Alexis wound retractor, Applied Medical, Rancho Santa Margarita, CA, USA) was inserted. A glove port was constructed. The tips of the thumb, the third, and the fifth finger of the glove were cut to open. One 12-mm-sized and 60-mm-long trocar and two 5-mm-sized and 55-mm-long trocars (Applied Medical) were inserted into the opened thumb and the other fingers of the glove, respectively and then tied with sterilized cable-tie. The glove port was placed all around and under the white ring of the wound retractor. The ring was everted until it was snugly tight to the abdominal wall. Pneumoperitoneum was created and laparoscopic exploration of the entire abdomen was carried out. The surgeon used all rigid, straight instruments, a 30-degree scope, and diathermy scissors or LigaSure Advance Instrument (Covidien, Mansfield, MA, USA) for dissection. The small bowel was displaced from the right side of the abdomen with the help of left-side tilt and Trendelenburg position of operation table. The surgeon adopted the lateral to medial and inferior to superior approach for ascending colon mobilization. Duodenum, right ureter, and gonadal vessels were preserved. Mobilization of the hepatic flexure and transverse colon was completed in reverse Trendelenburg position. All main vessels were divided intracorporealy. Ileocolic vessels and right colic vessels were divided individually at their origin. For RHC, the right branches of middle colic vessels were divided and for extended RHC, the main trunks of middle colic vessels were divided at their origin. Greater omentum was divided just distal to the gastroepiploic vessels. The glove port was removed to extract the specimen and perform the extracorporeal functional end-to-end ileocolic anastomoses using linear staplers. The incision was extended appropriately if the length of the incision was too small for specimen extraction. After hemostasis was ensured, a Jackson Pratt drain was inserted if indicated, the wound retractor was removed, and the wound was closed with absorbable sutures.
The technique of CL RHC was essentially similar to that used for SIL RHC except the ports placement. A 12-mm trocar was placed at subumbilicus for camera. Two 5-mm trocars were placed on the right abdomen, and another 5-mm trocar on the left lower abdomen and a 12-mm port on the left upper abdomen for instruments. The incision for the camera port was extended for specimen exteriorization and extracorporeal anastomoses.
Evaluation of learning curve and statistical analyses
Moving average of operative times
Moving average was used because trends in operating time may often not be clear due to fluctuations in operating time on a case-by-case basis. Because the moving average smoothes out short-term fluctuations and highlights the trends in time series data [3,5], it can be used to ascertain the end of the learning phase, which corresponds to the section of the graph where the curve reaches a plateau. In this study, the moving average of the order of 10 was used.
Mean operative time of every five consecutive cases
The mean operative time of every five consecutive cases were plotted against the corresponding number of cases performed, and the learning phase was considered overcome when the mean operative time reached a low point and subsequently did not vary by more than 30 minutes following the definition of Simons et al. [6].
Cumulative sum analysis
In this study, cumulative sum (CUSUM) analysis was used to chart major complications, namely anastomotic leakage, intraabdominal abscess or fluid collection, and postoperative bleeding. Bolsin and Colson [7] provided a summary of CUSUM analysis, and the following applications and methodology of CUSUM analysis are derived from their description.
To plot the CUSUM graph, four values have to be determined: s, 1-s, h0, and h1, where
s = Q/(P+Q) (s is the downward decrement with each success on a CUSUM plot, while the upward increment with each failure is 1-s); h0 = b/(P+Q) (h0 is the spacing between unacceptable boundary lines on the CUSUM graph); h1 = a/(P+Q) (h1 is the spacing between acceptable boundary lines on the CUSUM graph).
To obtain the four values, we need to first obtain P, Q, a, and b, where P = ln (p1/p0), Q = ln [(1-p0)/(1-p1)], a = ln [(1-β)/α], b = ln [(1-α)/β], p0 = acceptable failure rate, and p1 = unacceptable failure rate.
In this study, the acceptable failure rate was set to 5%. A p0 of 5% (0.05) was taken from the lowest overall complication rate [8] reported in the large systematic review by Tjandra and Chan [9]. We did not use a lowest overall complication rate of 0% because it is unrealistic and impractical to expect no complications at all during a surgeon's learning phase. p1 was set to 0.3, because 30% (0.3) was the approximate highest overall complication rate in the same review (actual value was 33%) [9].
α = type 1 error or failure rate (probability of wrongly accusing a trainee of unacceptable performance); β = type 2 error or failure rate (probability of wrongly certifying a trainee's performance as acceptable).
It is recommended to set α and β equally to 0.1 (10%) so that h0 and h1 are equal and the horizontal lines become equally spaced [10].
Therefore, in this study, h0 = h1 = 1.04, s = 0.15, and 1-s = 0.85. When the curve crosses the acceptable boundary (from above) or the unacceptable boundary (from below), the performance of the preceding series is considered acceptable or unacceptable, respectively, at the predefined acceptable failure rate of 5%, unacceptable failure rate of 30%, and types 1 and 2 error rates of 10%.
The CUSUM score is the running sum of a mixture of increments or 1-s (with each failure) and decrements or s (with each success). At the start of the series of analysis, CUSUM score C0 = 0, and thereafter, Cn is the CUSUM score of the nth procedure [7].
Data were analyzed using the t-test, Mann-Whitney test, Pearson chi-square test, or Fisher exact test as appropriate. A difference between groups was considered to be significant when the P-value was less than 0.05. Three methods were used to evaluate the learning curves of CL and SIL RHC.
RESULTS
Thirty five patients in the SIL RHC group and 29 patients in the CL RHC group were compared, because six cases with missing data in the CL RHC group were excluded from the analyses. Demographic and clinical data are summarized in Table 1, and operative results and early oncological and surgical outcomes are summarized in Table 2. Four out of the total 64 patients (6.3%) presented with intestinal obstruction caused by the primary cancer. Three patients were from the CL group and one patient was from the SIL group. One patient from the CL RHC group had undergone colonic stenting successfully for obstructing transverse colon cancer 4 days prior to the operation.
There were three cases with less than 12 harvested lymph nodes in the CL RHC group compared with one case in the SIL RHC group, but this difference was not statistically significant. The mean distal resection margin of SIL RHC was significantly longer than that of CL RHC, and this finding was correlated with a significantly larger number of the cases with extended RHC in the SIL group (Table 2).
The overall complication rate of SIL RHC was higher than that of CL RHC, but this difference did not reach statistical significance (Table 2). Postoperative bleeding in the CL RHC group was possibly due to bleeding from the anastomotic site, which was managed by conservative management. In the SIL RHC group, one of the two patients with postoperative bleeding was required reoperation. There was one case of intraabdominal fluid collection that was successfully treated by percutaneous drainage. Lymphorrhoea occurred in one patient of the SIL RHC group. It was spontaneously resolved by keeping a drainage catheter in place for a few days until the effluent was minimal.
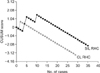
When the learning curve was evaluated with moving average of operation time with the order of 10, it started to flatten out at case number 31 for SIL RHC, while at case number 25 for CL RHC (Fig. 1). Because the trend of the initial part of any moving average graph is inevitably missing, we showed mean operative time of the every five consecutive cases. It reached the low point which did not vary by more than 30 minutes between case number 26 and 30 for SIL RHC, whereas between case number 16 and 20 for CL RHC (Fig. 2).
The CUSUM curve of CL RHC shown in Fig. 3 indicated that the surgeon had one case of postoperative bleeding (second case), which gave rise to an upward deflection. In subsequent cases, the curve crossed four acceptable boundaries (crossed four horizontal lines from above), indicating that the surgeon had four series of good performance. In other words, the surgeon demonstrated highly acceptable performance as early as his third case onwards. For SIL RHC, the surgeon had two consecutive complications in his 4th and 5th cases, which resulted in a long, upward curve that crossed two unacceptable boundaries (curve crossed two horizontal lines from below) followed by crossing an acceptable boundary with his four subsequent cases. However, another complication occurred in case number 10, which gave rise to an upward deflection that crossed an unacceptable boundary. Thereafter, the surgeon demonstrated highly acceptable performance. A comparison of both CUSUM curves indicated that more SIL RHC cases than CL RHC cases were required to reach a state of uninterrupted good performance.
DISCUSSION
Single-incision laparoscopic colectomy has been received with great interest among some colorectal surgeons, although the advantages of SIL over CL colectomy still have to be proven. Like many other new procedures, SIL colectomy has its own learning curve that needs to be overcome, and an evaluation of the nature of this learning curve will give surgeons some ideas of the number of cases, resources, and time required to overcome the learning phase. It may also be useful for planning training programs for the procedure [3] and designing clinical trials [5].
Moving average of operative times [3,5], mean operative time of every five consecutive cases [1,6], and CUSUM analysis [3,4,5] are some of the common methods that have been adopted to evaluate the learning curve of laparoscopic colorectal surgery. CUSUM analysis has been used in the several studies to assess the learning curve of CL colorectal surgery [3,4,5]; these studies used CUSUM analysis to study incompetence in terms of the adequacy of lymph node harvest, complication rate, conversion, or a combination of these markers of incompetence. However, we used only predefined complications as markers because there were no conversions in either group of patients and only one case of inadequate lymph node harvest in the SIL RHC group. Apart from allowing good assessment of the learning curve, CUSUM analysis, which was initially developed as a quality control test for production lines [8], can also be used as a monitoring tool to allow timely corrective measures to be made to prevent subsequent patients from being harmed by substandard performance [11]. As shown in this study, CUSUM curves can be used to monitor performance throughout the learning phase of the procedure so as to meet this objective. CUSUM analysis is suitable for those procedures that are performed frequently, have clearly defined success and failure criteria that are closely related to the surgeon's skill, and well-defined complications [11]. This study meets these criteria because the surgeon performed SIL RHC regularly and the relevant criteria were clearly defined.
The moving average method, which is a common tool used to monitor trends in financial data, has recently been adopted as a modality to assess the learning curve of laparoscopic colorectal surgery [3,5]. Because moving average analysis inevitably sacrifices data (in this study, operative time) of the initial part of the series, we also performed an analysis of the mean operative time of every five consecutive cases to address this shortcoming. Moving average of the order of 10 was used because the curve started to smooth out at this and a clear trend in operative time was discernable.
The significantly longer mean distal pathological margin in the SIL RHC group can be explained by the fact that there were significantly more cases of extended right hemicolectomies performed in the SIL RHC group than the CL RHC group. The presence of at least 12 lymph nodes in the surgical specimen is widely accepted as the standard of treatment in colorectal cancer. In this study, there were three cases (with six, eight, and 10 lymph nodes) in the CL RHC group and one case (with 10 lymph nodes) in the SIL RHC group with an inadequate number of harvested lymph nodes. However, the overall percentage of cases for which adequate lymph nodes were harvested (60 of 64 cases or 93.8%) in this relatively small study is more than that reported in the National Comprehensive Cancer Network (92%) and Surveillance Epidemiology and End Result (58%) databases, respectively [12].
In this study, three patients in the CL group and one patient in the SIL group with colonic obstruction were treated successfully with laparoscopic resection. This result is consistent with a study by Ng et al. [13]. who showed that laparoscopic-assisted RHC for obstructing right-sided colonic carcinoma is feasible and safe.
The reported mean operative time of CL RHC ranges widely between 107 and 208 minutes [14], while that of SIL RHC ranges between 75 and 166 minutes [15]. In the present study, the mean operative times for both SIL and CL RHC were within these reported ranges. However, it is noteworthy that this series included many challenging cases such as patients with a history of abdominal operation, bowel obstruction, or obesity, and all patients had malignant tumors. Despite these challenges, the overall lymph node yields in both groups were generally acceptable and the complication rate of SIL RHC of 17.1% in this relatively small study was less than the 21% reported for CL in some large clinical trials [16,17].
The learning phase for CL RHC in this study as determined by the moving average of the operative time and mean operative time of five consecutive cases was approximately 25 cases and between 16 and 20 cases, respectively, which falls within the range of between 11 and 70 cases reported by other studies for CL colorectal surgery [3]. In contrast, the learning phase for SIL RHC was approximately 31 cases, and between 26 and 30 cases based on the moving average of the operative time and mean operative time of five consecutive cases, respectively. As expected, the learning phase of both SIL RHC and CL RHC as determined by moving average analysis was longer than that determined by analysis of mean operative time of every five consecutive cases. This is probably because the moving average analysis inherently lags behind the latest data point, which is a drawback of the 'smoothing' effect of the moving average. Nevertheless, in both methods of analysis of the learning curve, the learning phase of SIL RHC was consistently longer than that of CL RHC.
Although there were no cases of conversion in this study, we do not view conversion as a failure. This is because conversion depends on the surgeon's case selection criteria, and does not necessarily indicate failure or incompetence [18], but may rather be a sign of maturity of surgical judgment [6]. Furthermore, in the event of conversion, there is the option of conversion into CL surgery by creating additional lateral ports [19], or hand-assisted laparoscopic surgery before considering proceeding to conventional open surgery.
Regarding the technical aspects of SIL RHC, we prefer a self-made glove port to some of the commercially manufactured single port devices because, in our experience, the range of axial movement of the rigid straight instruments is wider and there is less clashing of instruments at the port site when using a self-made glove port. This self-made glove port has also been reported to be appropriate and cost-effective in various operations [20]. Straight, rigid instruments are preferred over articulating instruments because, in our opinion, there is no need for adaptation of visual-spatial coordination for new articulating instruments. We prefer a lateral to medial approach as the correct plane of dissection is defined immediately once an incision is made along the white line of Toldt. With some of the manufactured single port devices, we find it difficult to adopt the lateral to medial approach because of limitations in the axial movement of the instruments at the port site.
Our results suggest that the learning phase of SIL RHC is longer than that of CL RHC. Early oncological outcomes and postoperative surgical outcomes of SIL and CL RHC based on the initial experience were comparable. Although SIL RHC had a higher complication rate than CL RHC during the learning phase, this was not statistically significant.




 XML Download
XML Download