

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Type II endoleak is the most common complication after endovascular aneurysm repair (EVAR) which could lead to a possible risk of aneurysmal sac enlargement and rupture [1]. If the sac is enlarged, surgical intervention might be needed. Many techniques have been described to treat type II endoleak. Transarterial embolization is usually used to treat type II endoleak. However, when standard trans-arterial treatment is not accessible, direct percutaneous sac injection (DPSI) is a good option [2]. Cone beam CT is very good option to guide DPSI. Here we report two cases of DPSI assisted by cone beam CT.
CASE REPORTS
Case 1
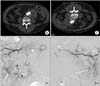
A 79-year-old male with a history of diabetes mellitus for 20 years and hypertension for 3 years had a 64 × 59-mm-sized infrarenal fusiform abdominal aortic aneurysm which was found during a regular physical checkup. The patient underwent elective EVAR using Excluder (W.L. Gore and Associates, Flagstaff, AZ, USA). Final angiogram after EVAR showed small amount of type II endoleak from lumbar arteries. Follow-up CT angiography at 6 months showed widening of preexisted type II endoleak. Therefore we performed translumbar arterial embolization for treatment of type II endoleak. However, this attempt failed due to tortuous collateral branches of lumbar artery. Therefore, we performed DPSI. The patient was placed in the prone position. The best route o f approach was defined using cone beam CT (Xpert CT, Philips, Best, The Netherlands) (Fig. 1). After local anesthesia, a 21-gauge Chiba needle was inserted through paraspinal route directly into type II endoleak sac under fluoroscopy guidance. Then 2 mL of glue mixed in 4 mL of Lipidol was injected into the type II endoleak sac. The procedure was finished without any complications. Six month CT follow-up showed no signs of recurrent type II endoleak.
Case 2
A 72-year-old female with a history of diabetes mellitus for 4 years, hypertension for 10 years, and angina pectoris for 6 years had a 55 × 45-mm-sized infrarenal abdominal aortic aneurysm during a regular physical checkup. The patient underwent elective EVAR using Excluder (W.L. Gore and Associates, Flagstaff). At the end of EVAR, we founded type II endoleak from lumbar arteries. The patient complained abdominal pain and the aneurysm sac became larger than the initial diameter (58 mm × 59 mm) at 38 months post operation. We decided to perform embolization of arteries for treatment of type II endoleak. However, there was no route to approach the lumbar arteries. Therefore, we decided to perform DPSI. The patient was placed in the prone position. The best route of approach was defined using cone beam CT (Xpert CT, Philips). After local anesthesia, a 21-gauge Chiba needle was inserted through paraspinal route directly into type II endoleak sac under fluoroscopy guidance. Then we confirmed the placement of needle using cone beam CT. Then 2 mL of glue mixed in 4 mL of Lipidol was injected into the type II endoleak sac (Fig. 2). The procedure was finished without any complication. Six-month CT follow-up showed no signs of recurrent type II endoleak.
DISCUSSION
Cone beam CT, a method to acquire image using cone beam shaped ionized radiation, is usually used in industrial and biomedical area to easily obtain 3-dimensional (3D) images [3]. Since its original development in 1984, cone-beam algorism enables reconstruction and modification of 3D image data [4]. This technology is usually used in many kinds of industrial and medical applications. Single photon emission computerized tomography, angiography, and radiotherapy were examples of various medical applications of cone-beam CT. The advantages of cone-beam CT include its ability to measure accurately, improve localization, identify and quantify asymmetry, visualize anatomic abnormalities, assess target structures, identify bony structures, and plan placement sites for devices. All these will add knowledge base to the practitioner at the time of diagnosis. Therefore, cone-beam CT could help physicians with risk assessment by assessing target structure, visualizing placement of devices, and providing the imaging data to support treatment simulation and technology-aided treatment [5]. Type II endoleaks is the most common complication after EVAR. In most cases, this complication was observed without any management. If type II endoleak caused continued sac expansion and potential sac rupture, surgical repair such as transarterial embolization is needed. Inferior mesenteric artery, internal iliac artery or lumbar artery is usually selected as the route for transarterial embolization. If there are no arterial routes for transarterial embolization, DPSI is feasible as an alternative method to treatm type II endoleak. However, DPSI needs very precise measurement to avoid puncture of inferior vena cava or vessel around sac or stent graft. In this situation, cone beam CT is very useful to easily obtain 3D images. We used DPSI for the two cases described here. For case 1, we made the decision of using DPSI and cone beam CT on the second day after trying transarterial embolization on the first day. For case 2, we made the decision of using DPSI immediately after realizing no route for transarterial embolization because we had the experience of DPSI using cone beam CT. In the two cases described above, cone beam CT was successfully used to find the exact position of the needle and guide needle injection for DPSI. Therefore, cone beam CT is a useful tool to evaluate needle position and circumference anatomy for DPSI to treat endoleaks after EVAR.
 XML Download
XML Download