

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nonincisional lateral abdominal wall hernia (LAWH) is a very rare condition, although incisional hernias along the lateral abdominal wall incision can occur infrequently [1,2]. LAWH has to be differentiated from other rare types of hernias such as lumbar hernia or spigelian hernia. We experienced an unusual type of nonincisional LAWH in a 68-year-old woman, which was located at the right flank just below the costal margin and was not associated with any suspected causes of hernia such as trauma or infection. Its location is different from that of spigelian hernia or lumbar hernia. We report here this rare case of nonincisional LAWH that was treated by laparoscopic mesh repair with a review of relevant literatures.
CASE REPORT
A 68-year-old woman visited our outpatient clinic after suffering abdominal discomfort with a bulging mass at the right flank. She was 156 cm tall and weighed 60 kg with a body mass index score of 24.7 kg/m2. She was a smoker and had a 20-pack-a-year history. She found the mass upon heavy coughing 3 months prior. The past medical history did not reveal any previous abdominal trauma, infection, or operation. She underwent a total thyroidectomy for papillary thyroid microcarcinoma (T1N1M0) 13 years prior and has been followed up without evidence of recurrence. She has taken levothyroxine after total thyroidectomy and steroid medication for rheumatoid arthritis for a long time.
Physical examination showed a large protruding mass measuring 8 cm in diameter in the midaxillary line just below the costal margin on her right flank during valsalva maneuver. It disappeared by changing position to the left lateral decubitus or by manual reduction. All results of preoperative laboratory tests were within normal ranges except suppressed serum TSH concentration. Findings in chest x-ray and echocardiography were normal. Abdominopelvic CT scan showed omental fat herniation through a lateral abdominal wall defect of the transversus abdominis muscle and internal oblique muscle at the right flank (Fig. 1).
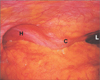
We performed laparoscopic hernia repair using 20 × 15-cm-sized Parietex composite mesh (Covidien, Seoul, Korea) with an intraperitoneal onlay mesh technique. Laparoscopic exploration of the abdomen revealed omental herniation through the lateral abdominal wall defect measuring 6.5 cm × 6 cm (Fig. 2). The right colon was mobilized at the hepatic flexure to provide adequate margins, at least 4 cm, surrounding the defect for mesh placement. The peritoneum overlying the hernia was dissected off and the mesh was positioned over the defect with 4-cm margins and secured with transmural nonabsorbable sutures and intra-abdominal tacks. The patient had an uneventful postoperative course and was discharged. There is no evidence of hernia recurrence at 6-month and 1-year follow-up visits.
DISCUSSION
There are various types of abdominal wall hernias. Common types of hernias such as inguinal hernia, femoral hernia, and umbilical hernia can be diagnosed easily by their locations. However, LAWH is rare. Differential diagnoses of this condition involve rare types of hernias such as lumbar hernia or spigelian hernia. Incisional hernias or traumatic hernias can also be developed, though rarely, in the lateral abdominal wall [3]. Nonincisional or nontraumatic LAWH is an extremely rare condition.
We experienced an unusual type of LAWH in a 68-year-old woman, which was located at the right flank just below the rib cage and was not associated with trauma or infection. There was a defect in the transversus abdominis muscle and the internal oblique muscle in the midaxillary line just below the costal margin at the right flank. The case was quite different from lumbar hernia or spigelian hernia in its anatomic location.
Spigelian hernia constitutes only 0.12% of all abdominal wall hernias [4]. It is also known as 'spontaneous lateral ventral hernia' or 'hernia of semilunar line'. Spigelian hernia is a defect in the anterior abdominal wall beside the semilunar line. Most of these hernias lie in the spigelian hernia belt, a transverse 6-cm-wide zone above the interspinal plane. The present case is not located on the Spigelian hernia belt.
Lumbar hernias are rare posterolateral abdominal wall hernias. Primary lumbar hernias are classified into two types according to the location: the superior lumbar hernia (Grynfeltt) and the inferior lumbar hernia (Petit) [1]. They develop through the superior and inferior lumbar triangles. The superior lumbar triangle is bordered by the quadratus lumborum muscle medially, the posterior border of the internal oblique muscle inferiorly, and the 12th rib superiorly. The inferior lumbar triangle is bordered by the iliac crest inferiorly, the latissimus dorsi medially, and the external oblique muscle laterally. In the aspect of location, the present case is different from typical primary lumbar hernias.
In the literature, to our knowledge, Castillo-Sang et al. [2] only reported a similar type of hernia like the present case. They reported a 56-year-old male who presented a right lateral abdominal wall bulge in the midaxillary line immediately below the rib cage. The patient had no history of trauma or surgery. The hernia defect was bordered by the inferior aspect of the 11th rib superiorly and a bony spur descending from the inferior portion of the 11th rib and a defect in the transversus abdominis and internal oblique muscles laterally. A bony spur arising from the 11th rib suggested a congenital etiology. The authors claimed that it was the first report of a nontraumatic, LAWH in an adult. We think this is the first report of this kind of hernia in Korea and may be the second report in the literature. In the present case, however, the lateral abdominal bulge appeared suddenly after heavy coughing. Abdominal wall hernias can be developed by multifactorial causes [5]. Our patient had several risk factors of hernia development. Coughing can increase intra-abdominal pressure. Aging, long-term medication of steroids and smoking can weaken the abdominal wall. Actually, Lund et al. [6] reported a posterolateral abdominal wall hernia secondary to a severe cough spells. However, the hernia was located at a more posterior position than the present case.
Since the first reports of successful laparoscopic repairs of lumbar hernia in the late 1990s by several groups, many surgeons prefer a laparoscopic approach for lumbar hernia [7,8]. Laparoscopic hernia repair is also very useful for lateral ventral wall hernia [2,9]. We also performed laparoscopic hernia repair using a composite mesh with an intraperitoneal onlay mesh technique. The patient had an uneventful postoperative course and was discharged. There is no evidence of hernia recurrence at 6-month and 1-year follow-up visits.
Here we reported a very rare case of a nonincisional, LAWH in an adult. Its location is different from other rare type of abdominal wall hernias. There was no history of trauma or surgery as the etiological factor but severe coughing might influence hernia development. Laparoscopic repair spared the patient a larger incision and associated comorbidities.

 XML Download
XML Download